Key Points
- Neuromuscular blocking agents (NMBAs) work at the neuromuscular junction (NMJ) to inhibit the nicotinic receptor. There are two types: depolarizing and nondepolarizing NMBAs.
- ED95 is the dose of an NMBA required to produce an effect (95% suppression of a single-twitch response). It is referred to as the “effective dose” and used as a measure of potency.
- Differences in body composition and metabolism impact neuromuscular blockade dosing and duration in children.
- Neonates and infants require smaller doses of nondepolarizing NMBAs and less frequent redosing. However, the onset of action is faster.
Mechanisms
Mechanism of Muscle Relaxation
- When a nerve impulse arrives at the NMJ, voltage-gated Na+ channels open, leading to an influx of calcium within the terminal. This causes several hundreds of vesicles of acetylcholine (ACh) to fuse with the nerve membrane. The ACh within these vesicles is released into the synaptic cleft, where they combine with and activate nicotinic receptors on the motor endplate. This activation opens the ion channel on the muscle membrane and depolarizes the muscle fiber membrane1-3 (Figure 1).
- Please see the OA Summary on the basics of neuromuscular blockade for more details. Link

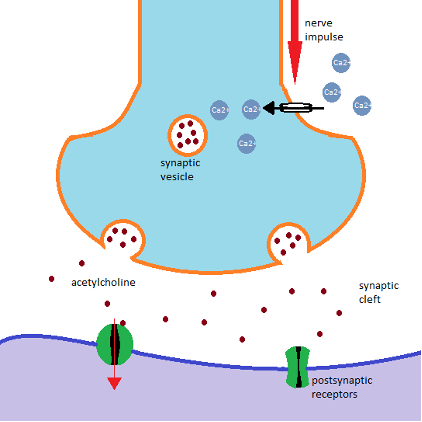
Figure 1. Mechanism of action of neuromuscular blocking agents
NMBAs
- NMBAs work at the NMJ to inhibit the nicotinic receptor. There are two types: depolarizing and nondepolarizing.
Depolarizing NMBAs are ACh receptor agonists. They bind to ACh receptors and cause a depolarization of the endplate which leads to rapid skeletal muscle relaxation. In this state, the endplate cannot repolarize, resulting in a phase I block. The duration of action is brief, due to their hydrolysis by plasma cholinesterase (pseudocholinesterase/butyrylcholinesterase). The rapid breakdown of succinylcholine allows only a fraction of the administered dose to reach the NMJ. There is little to no plasma cholinesterase at the NMJ, so the action of succinylcholine is terminated by diffusion from the endplate to the extracellular fluid. By controlling the rate at which succinylcholine is hydrolyzed before it reaches, and after it leaves the NMJ, plasma esterase influences the onset and duration of action of the drug.1-3 - Nondepolarizing NMBAs are competitive antagonists which means they bind to the ACh receptor and prevent ACh from binding. However, endplate depolarization does not occur as they are unable to induce ion channel openings. They may also be capable of directly blocking the ion channel, stopping the flux of Na+ through the ion pore, which interferes with mobilization of ACh from their sites of synthesis.1-3
- Upregulation of ACh Receptor sites results in increased sensitivity to depolarizing NMBAs and resistance to nondepolarizing NMBAs.
- Example states: Upper and lower motor neuron lesions, burns, severe infection, prolonged use of neuromuscular blocking agents, muscle trauma, cerebral palsy, and chronic use of anticonvulsant agents
- Downregulation of ACh Receptor sites results in resistance to depolarizing NMBAs and increased sensitivity to nondepolarizing NMBAs.
- Example states: myasthenia gravis, organophosphate poisoning, and exercise conditioning
ED95
- ED95 refers to the amount of NMBA required to reduce twitch height by 95%.1,2
- The dose of an NMBA required to produce an effect (95% suppression of a single-twitch response) is referred to as the “effective dose” and is used as a measure of potency.
- One to two times the ED95 is usually used for intubation. The ED95 of commonly used NMBAs is listed in Table 1.

Table 1. Commonly used NMBAs with their ED95 and induction doses
Fade
- Tetanic stimulation = 5 seconds at 50-100 Hz
- Tetanic stimulation causes massive release of ACh at the NMJ and strong muscle contraction.
- Tetanic fade (progressive weakening) occurs with tetanic stimulation, likely via a presynaptic mechanism. The nerve initially dumps large volumes of ACh into the NMJ. The total amount of ACh released from the presynaptic nerve decreases over time, and eventually equalizes with the amount of ACh the nerve produces. Fade is not detectable because the amount of ACh being released is substantially greater than what is needed to depolarize the motor endplate.1
- Fade occurs with tetanic stimulation in the presence of nondepolarizing NMBAs. The nondepolarizing NMBA acts as a competitive inhibitor of ACh leading to decreased effect of ACh in the NMJ. NMBAs may also work on the presynaptic nerve fiber by binding to presynaptic ACh receptors thereby decreasing ACh mobilization.1
- Fade can also be seen when the number of ACh receptors is reduced, such as in myasthenia gravis.1,2
- When the train-of-four ratio is greater than 0.4, it is difficult to evaluate fade either manually or visually.2
- Depolarizing NMBAs cause phase I block resulting in a significantly attenuated response to tetanus; however, no fade occurs.
Synergism
- When the effect of two drugs is greater than the sum of the two drugs, it’s called synergism. Nondepolarizing NBMAs are synergistic when drugs of different structural classes are combined. For example, cisatracurium and vecuronium administered together increase the depth of blockade as does cisatracurium and mivacurium but to a lesser extent.
- Both the depth and the length of the block may be prolonged. The precise mechanism of synergism is not known. When drugs from the same structural class are given, the effect is additive, not synergistic.1
Neuromuscular Blockade in Children
- Differences in body composition and metabolism impact neuromuscular blockade dosing and duration in children. Induction doses for infants and children are shown in Table 2.2
- Neonates and infants have immature muscular transmission, requiring smaller doses of nondepolarizing NMBAs.
- Neonates and infants have higher cardiac output per kilogram, leading to faster onset times.
- Neonates and infants have immature kidney and liver function causing prolonged metabolism and clearance of most NMBAs. This results in less frequent redosing.
- In summary, neonates and infants require smaller doses of nondepolarizing NMBAs and less frequent redosing. However, the onset of action is faster.
- Infants have an increased total body water and extracellular fluid compartment compared to adults, creating a larger volume of distribution and a higher dose requirement for succinylcholine.
- Compared to infants, children have increased muscle bulk with more ACh receptors, requiring larger induction doses.
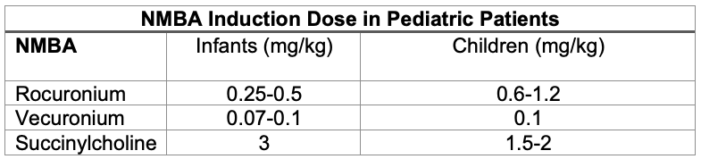
Table 2. Intravenous induction doses of NMBAs in infants and children
- Caution should be used with succinylcholine as it may activate cardiac muscarinic ACh receptors in the sinus node leading to arrhythmias including bradycardia and asystole.2
- Additionally, caution should be used in pediatric patients due to the risk of life-threatening hyperkalemic rhabdomyolysis in patients with undiagnosed skeletal muscle myopathy, most frequently Duchenne’s muscular dystrophy.2
References
- Brull SJ, Meistelman C. Pharmacology of neuromuscular blocking drugs. In: Gropper MA, et al (eds): Miller's Anesthesia. 9th edition Philadelphia, PA. Elsevier; 2019. 792-831.
- Weigel WA, Grant SA, Thilen SR. Neuromuscular blocking drugs. In: Barash, Cullen, and Stoelting’s Clinical anesthesia. 9th edition, Philadelphia, PA. Wolters Kluwer. 2023.
- Martyn JA, Fagerlund MJ, Eriksson LI. Basic principles of neuromuscular transmission. Anaesthesia. 2009;64 Suppl 1:1-9. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.