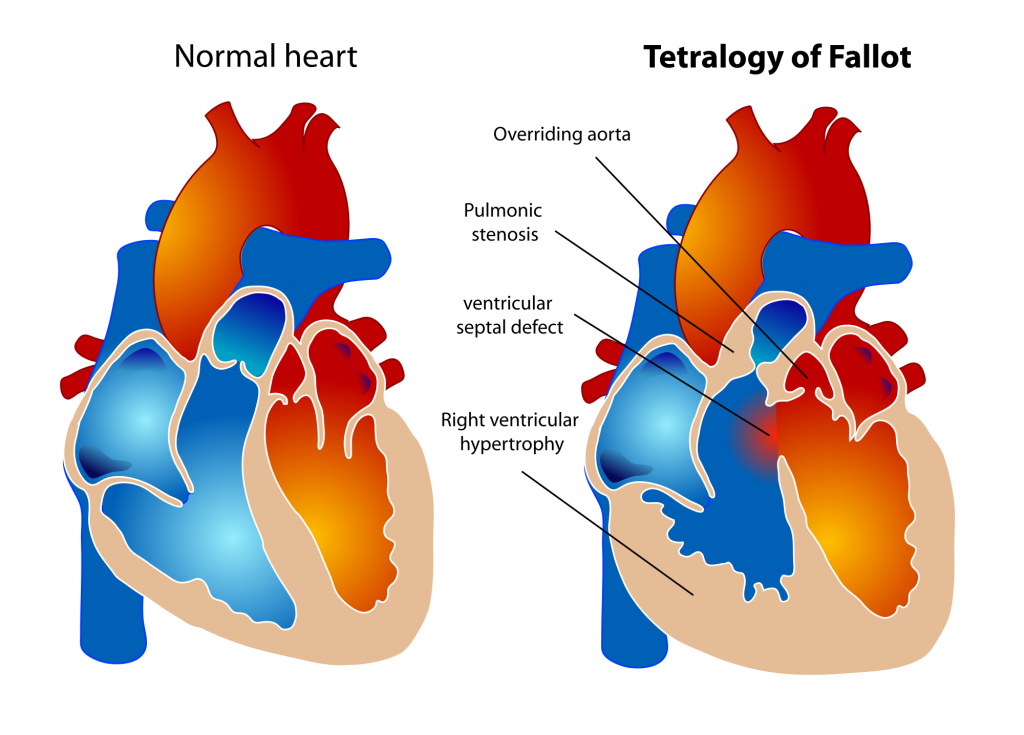
Tetrology of Fallot usually consists of right ventricular obstruction, right ventricular hypertrophy, and a VSD with an over-riding aorta. The right ventricular obstruction is usually secondary to hypertrophy of the subpulmonic muscle. Up to 25% of patients also have pulmonic stenosis. The infundibular obstruction dynamic and can be increased secondary to sympathetic tone, this obstruction is responsible for “tet spells” or the hypercyanotic spells seen in young patients.
The combination of the right ventricular obstruction with the VSD leads to a large right to left shunt. This shunt is composed of a fixed component and variable factors (fixed= severity of right ventricular obstruction, variable = SVR and PVR). Surgical management often includes a modified Blalock-Taussig (left subclavian to pulmonary artery shunt), with correction of the VSD, and repair or replacement of the pulmonic valve, and removal of obstructing infundibular muscle.
Anesthetic objectives for patient’s with Tetrology of Fallot: maintain intravascular volume and SVR. Avoid increases in PVR as may be caused by acidosis or increased airway pressures. Drugs such as Ketamine are recommended for induction because ketamine increases SVR and does not increase the right to left shunting. Of note, the right to left shunt tends to slow the rate of rise of inhalational agents. Conversely, the right to left shunt may speed the onset of intravenous agents. Oxygenation may improve after induction. Avoid muscle relaxants that release histamine. Cyanotic spells can be treated with volume and phenylephrine (5micrograms/kg). Propranolol may help to relieve infundibular spasm. If hypoxemia is severe, correcting the resulting acidosis may be necessary with sodium bicarbonate.

Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.