TCAs have diverse mechanisms of action which accounts for the wide array of symptoms that can present in an overdose situation. An overdose can occur following intentional excess ingestion or due to drug-drug interactions or pharmacogenetic variations. Doxepin is metabolized by the CYP2D6 enzyme and tertiary amine TCAs such as amitriptyline, imipramine, and clomipramine are metabolized by other CYP enzymes and any genetic or pharmacologic inhibition of these enzymes could potentially result in high plasma levels of these drugs.
TCA overdose can initially manifest with anticholinergic symptoms such: dry mouth, change in mental status, tachycardia and urinary retention, Pupils are generally constricted due to the alpha effects of TCAs and patient can be hypertensive or hypotensive due to inhibition of norepinephrine reuptake or norepinephrine store depletion respectively. Seizures are not uncommon due the variety of receptors that TCAs act on. Late in the overdose sodium channel blockade can result in bradycardia and hypotension.
TCA overdose and the resultant sodium channel and potassium channel blockade can result in QRS and QT prolongation respectively. In severe cases of overdose, these prolongations can result in wide-complex arrhythmias. Other ECG findings seen in TCA toxicity include a terminal R wave (R’) in aVR >3mm and a R:S ratio in aVR > 0.7
Treatment for TCA overdose without ECG abnormalities is supportive with benzodiazepines or antiepileptics used to treat seizures. Of note, caution should be used in treating these patients with physostigmine (a typical antidote for pure anticholinergic poisoning) due to reports of asystole in patients with TCA toxicity. If there is evidence of significant sodium channel blockade (i.e. wide QRS), treatment includes hypertonic sodium bicarbonatein an effort to alkalinize the plasma and counteract the sodium channel blockade effects. An infusion should be titrated to QRS duration and a pH of 7.5 to 7.55.

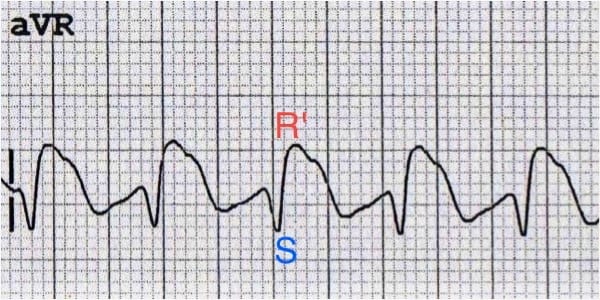
Fig 1: ECG tracing of aVR showing wide QRS and terminal R' wave >3mm.
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.