Key Points
- Pseudocholinesterase (PChE) metabolizes succinylcholine, mivacurium, and ester local anesthetics. Different molecular forms result in varying levels of enzyme activity.
- PChE deficiency causes a reduced ability to metabolize those drugs.
- PChE deficiency is inherited in an autosomal recessive manner.
- To rule out PChE deficiency, recovery of neuromuscular function must be documented after succinylcholine administration and before administering a nondepolarizing neuromuscular blocking agent.
Pseudocholinesterase
- Pseudocholinesterase (PChE) is a serine hydrolase that catalyzes the hydrolysis of choline esters.1 Pseudocholinesterase is also called plasma cholinesterase, serum cholinesterase, acetylcholine acetylhydrolase, and butyrylcholinesterase (BuChE).2
- There are different molecular forms of BuChE built from identical subunits.1 The symmetric monomeric form is called G1, and the diametric form is called G2. G2 consists of two molecules joined by a disulfide bridge between the cysteine residues of each monomer.
The G4 form is a tetramer consisting of two G2 forms held together by hydrophobic interactions. - PChE is synthesized in the liver. The enzyme can be found in the kidneys, pancreas, nervous system (including the brain), and plasma. Its serum half-life is 8 to 12 days.
- The gene that codes for BuChE is located on chromosome 3q26. The gene spans about 70 kb and has four exons and three introns. More than 40 mutations/variants of BuChE have been recognized, each with different activity levels.
Function of Pseudocholinesterase
- PChE influences neurons in the hippocampus, amygdala, thalamus, and cerebral cortex.2
- It has a functional role in the maturation of the central and peripheral nervous system.
- The enzyme regulates neuronal growth and cell proliferation in the early stages of neuronal development.
- It also metabolizes succinylcholine, mivacurium, ester local anesthetics, and organophosphates (pesticides).1,2
- It may play a role in the development of Alzheimer’s disease, addiction pathophysiology, tumorigenesis, and other neuronal disorders.
- Serum levels of PChE may be a biomarker of liver function.
Variants of Pseudocholinesterase
- In patients with normal PChE activity, succinylcholine is rapidly hydrolyzed with a half-life of two to four minutes.
- Five alleles make up the variants of the PChE enzyme:6
- Wild type (U), normal
- Dibucaine resistant (A)
- Fluoride resistant (F)
- Silent (S)
- Kailow (K)
- Two copies of an altered allele must be present to result in a significant delay in enzyme activity. Mutations occur at a rate of one in 2,000 to 5,000 for homozygotes and one in 500 for heterozygotes.3-6
- When a mutation is present, succinylcholine’s action can be prolonged from 10 minutes to 8 hours or more (Table 1).
- Mutations are more common in certain populations.6
- Persian Jews
- White males of European descent
- Alaskan Inuits
- Arya Vysyas community in Andhra Pradesh, India
- There is a male-to-female ratio of 2:1.
- C5 is a variant allele of the pseudocholinesterase gene that increases enzymatic activity and succinylcholine resistance2.
- Resistance to succinylcholine caused by increased PChE activity has been seen in patients with:
- Hyperlipidemia
- Modular goiter
- Obesity
- Diabetes mellitus
- Psoriasis
- Hypertension
- Thyrotoxicosis
- Nephrosis
- Asthma
- Alcoholism
- Anxiety
- Schizophrenia

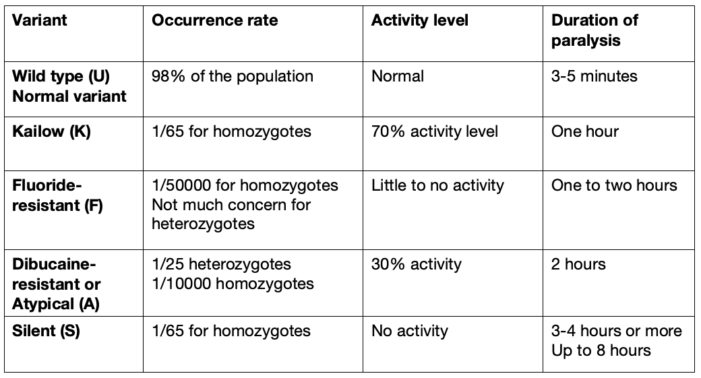
Table 1. PChE variants, occurrence, activity, and duration6
Causes of Pseudocholinesterase Deficiency
- Deficiency of PChE can be inherited (as an autosomal recessive trait), acquired, or iatrogenic.4,5
- Acquired deficiency can be due to:4,5
- Advanced age
- Pregnancy
- Kidney disease
- Malnutrition
- Liver disease
- Cancer
- Collagen vascular disease
- Burns
- Hypothyroidism.
- Iatrogenic causes are usually pharmaceutical agents that interfere with enzyme activity such as4,5
- Steroids
- Contraceptives
- Cytotoxic agents
- Anticholinergic drugs
- Echothiopate eye drops
- Organophosphate insecticides
- Monoamine oxidase inhibitors
- Anticholinesterase drugs
- Plasmapheresis can also deplete plasma cholinesterase levels.
Diagnosis
- Dibucaine is an amino amide local anesthetic that inhibits PChE.
- The dibucaine number identifies any variants of PChE deficiency by percent of inhibition:4,5
- Normal variant will have a dibucaine number of 80%, with a range of 71-85%
- Heterozygotes will have a 50-60% dibucaine number
- Homozygotes will have a 20-30% dibucaine number
- Enzyme level will also be diagnostic. Normal levels of PChE are between 2900-7100 U/L.
- The dibucaine number and pseudocholinesterase levels should be drawn for any patients with a suspected enzyme deficiency.
- Pseudocholinesterase levels should be drawn after a patient has full muscle recovery. Enzyme activity can be affected by the amount of anesthetic administered to the patient. The dibucaine number will not be affected.
- These tests are usually performed at outside laboratories.
- Family members should be tested as well.
Differential Diagnosis
- The differential diagnosis of PChE deficiency is broad and includes:4,5
- Narcotic overdose
- Myasthenia gravis
- Myasthenia crisis
- Hypermagnesemia
- Hypophosphatemia
- Hypokalemia
- Hypothermia can cause prolonged blockade.
- Phase II block- A train of four fade will be indicative.
Management
- There are no current treatments in the United States for PChE deficiency. The recommended management is supportive care, keeping the patient sedated and ventilated until spontaneous recovery. 4,5 Usually, the patient is transferred to the ICU intubated.
- Human plasma cholinesterase is available in Europe but is not commonly used. It has not shown to be very reliable.
- Plasma contains pseudocholinesterase. Transfusion of fresh frozen plasma (FFP) has been shown to increase a patient’s enzyme level and activity.
- Whole blood has pseudocholinesterase as well and can improve enzyme activity
- Transfusions of FFP and whole blood are not recommended treatments. The level of enzyme activity will vary per unit and there are no set guidelines on the number of units needed to reverse muscle blockade. This is not a good use of valuable blood products and poses a risk of iatrogenic infections.
- Administration of an anticholinesterase is not recommended. Administration has been shown to potentially transiently reverse the apneic effects of succinylcholine. However, this is followed by an intensified neuromuscular blockade.
- The potential for PChE enzyme deficiency makes it vital to check for recovery from succinylcholine before administering any other paralytic and waking up a patient.
References
- Darvesh S, Hopkins DA, Geula C. Neurobiology of butyrylcholinesterase. Nat Rev Neurosci. 2003 ;4(2) :131-8. PubMed
- Banner A, Lewallen FN, Sadiq NM. Biochemistry, Pseudocholinesterase. StatPearls. [Internet]. Treasure Island, FL. StatPearls Publishing; 2024 Jan. PubMed
- Alexander DR. Pseudocholinesterase deficiency. Medscape., Dec 2022. Link
- Juels A, Juels P. Pseudocholinesterase deficiency after multiple previous anesthetics. Anesthesiology News. 2021. Link
- Trujillo R, West WP. Pseudocholinesterase deficiency. StatPearls. [Internet]. Treasure Island, FL. StatPearls Publishing; 2022 Sep. Link
- Pandit JJ, Gopa D, Arora J. A hypothesis to explain the high prevalence of pseudocholinesterase deficiency in specific population groups. Eur J of Anaesthesiol. 2011; 28(8):550-2. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.