Key Points
- Pregnancy causes several physiologic changes in the cardiovascular system.
- Maternal cardiac output increases during the first and second trimesters.1,2
- An increase in heart rate contributes to most of the increase in cardiac output during the first trimester, whereas an increase in stroke volume contributes to most of the increase in cardiac output during the second trimester.2
- There are structural changes to the heart that occur to accommodate the changes in cardiac physiology. These changes are reflected in certain physical exam findings.
- Blood pressure (BP) and systemic vascular resistance (SVR) decrease during the first and second trimesters. BP goes back to prepregnancy values towards the end of the third trimester, but SVR remains approximately 20% below prepregnancy values at the end of pregnancy.1,2
Introduction
- Pregnancy involves complex physiological changes to adapt the body to carry a growing fetus. One of the most important systems affected by these physiological changes is the cardiovascular system.
- The changes that occur through the first, second, and third trimesters are important for an anesthesiologist to know, as some of these hemodynamic changes affect anesthetic management.
- This summary will cover the normal and abnormal changes of cardiovascular physiology in a pregnant patient.
Physiological Changes
Normal Changes
- Higher blood volume: Estrogen raises renin levels and leads to sodium and water retention through the renin-angiotensin aldosterone system.3
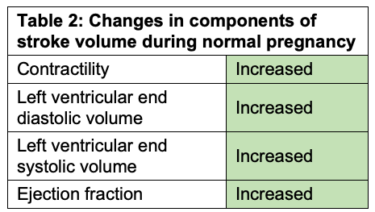
- Cardiac output (CO): Both heart rate and stroke volume increase throughout pregnancy. The initial increase in cardiac output in the first trimester is due to an increase in heart rate, whereas most of the increase in cardiac output in the second trimester is due to an increase in stroke volume.1,2
- The changes in CO, heart rate (HR), blood pressure (BP), and stroke volume (SV) in pregnancy are listed in Tables 1, 2, and 3.1,2

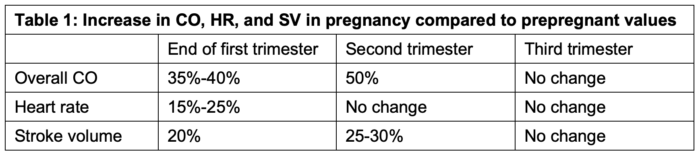
Abbreviations: CO, cardiac output; HR, heart rate; BP, blood pressure; SV, stroke volume
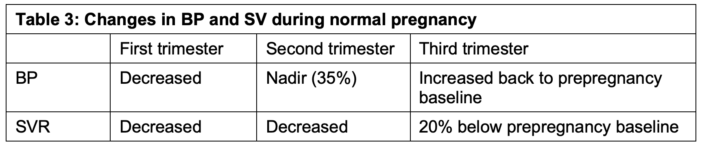
Abbreviations: BP, blood pressure; SVR, systemic vascular resistance
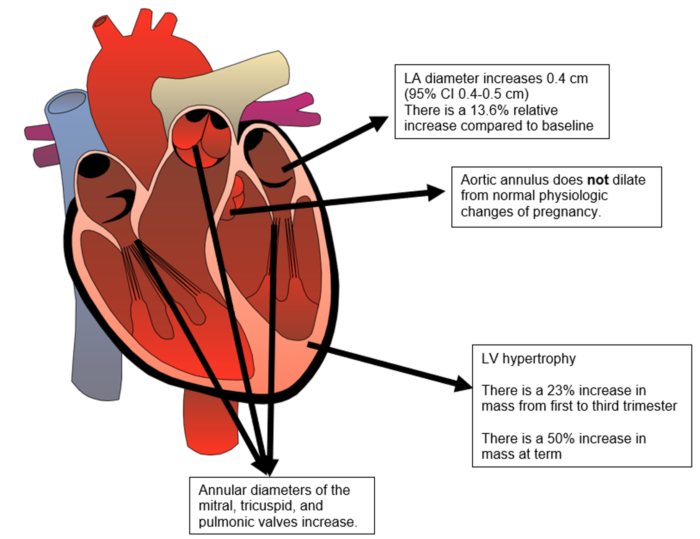
Figure 1. Structural changes of the heart during normal pregnancy. Abbreviations: LA, left atrium; LV, left ventricle. Adapted from ArtFavor. Medical illustration of a human heart. Public Domain. Link
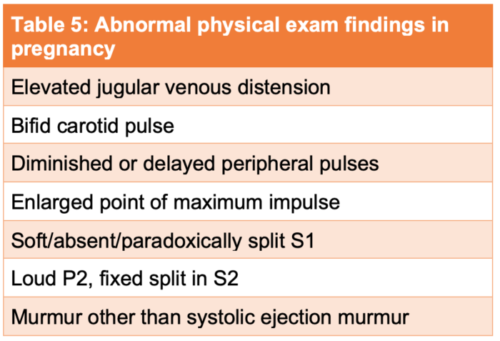
- Normal and abnormal physical exam and electrocardiogram (ECG) changes are listed in Tables 4 and 5.4-6
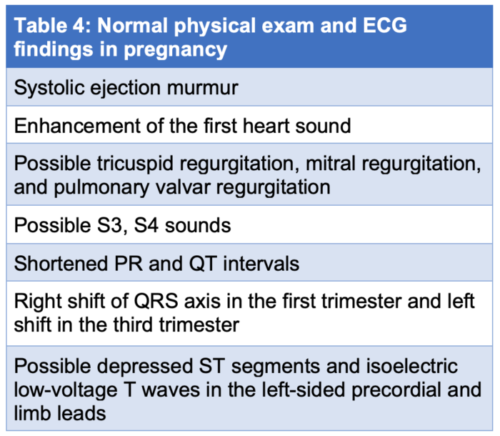
Abbreviations: ECG, electrocardiogram
Laboratory Testing
- Plasma lipid concentration increase
- Total serum cholesterol, triglycerides, LDL cholesterol concentrations all increase due to insulin resistance and increase in estrogen levels.7
- B-type natriuretic peptide (BNP)8
- Normal pregnancy has double the nonpregnant levels of BNP.
- The BNP levels does not change between trimesters.
- Cardiac enzymes
- Cardiac enzymes are not elevated above the upper limits of normal during normal pregnancy.9
- Troponin levels may be elevated in gestational hypertension or preeclampsia.10
- CK-MB levels can be elevated up 2-4 times due to the presence of these enzymes in uterus and placenta.11
Echocardiography Changes
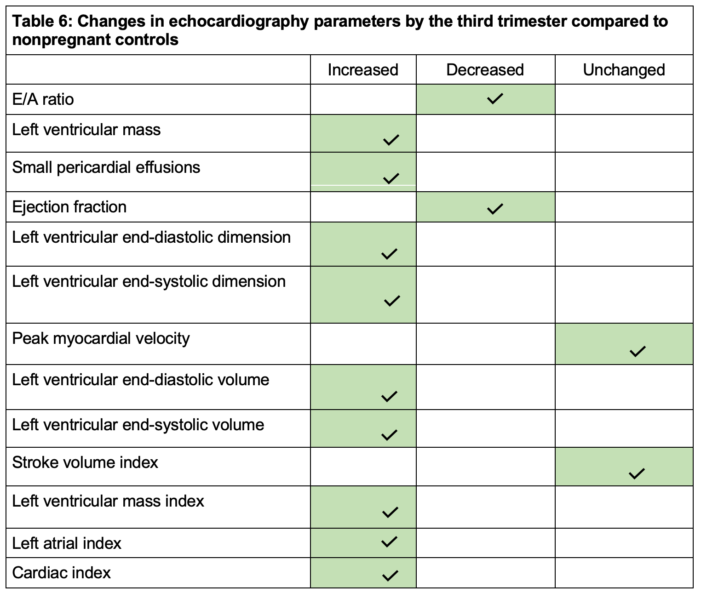
• Echocardiographic changes during pregnancy are listed in Table 6.12
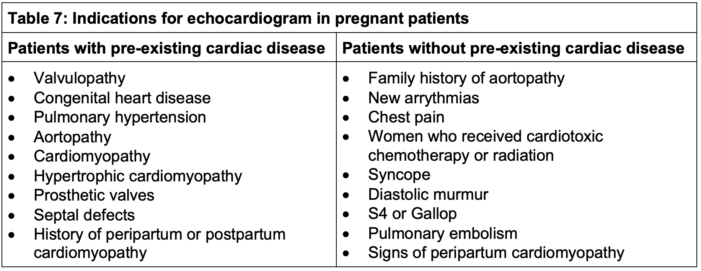
- Indications for echocardiography in pregnant patients are listed in Table 7.12
References
- Capeless EL, Clapp JF. Cardiovascular changes in early phase of pregnancy. Am J Obstet Gynecol. 1989;161(6 Pt 1):1449-53. PubMed
- Robson SC, Hunter S, Boys RJ, et al. Serial study of factors influencing changes in cardiac output during human pregnancy. Am J Physiol. 1989;256(4 Pt 2):H1060-5. PubMed
- Stachenfeld NS. Sex hormone effects on body fluid regulation. Exerc Sport Sci Rev. 2008;36(3):152-9. PubMed
- Cong J, Fan T, Yang X, et al. Structural and functional changes in maternal left ventricle during pregnancy: a three-dimensional speckle-tracking echocardiography study. Cardiovasc Ultrasound. 2015; 13:6. PubMed
- Carruth JE, Mivis SB, Brogan DR, Wenger NK. The electrocardiogram in normal pregnancy. Am Heart J. 1981;102(6 Pt 1):1075-8. PubMed
- Cutforth R, MacDonald CB. Heart sounds and murmurs in pregnancy. Am Heart J. 1966;71(6):741-7. PubMed
- Lippi G, Albiero A, Montagnana M, et al. Lipid and lipoprotein profile in physiological pregnancy. Clin Lab. 2007;53(3-4):173-7. PubMed
- Hameed AB, Chan K, Ghamsary M, Elkayam U. Longitudinal changes in the B-type natriuretic peptide levels in normal pregnancy and postpartum. Clin Cardiol. 2009;32(8): E60-E62. PubMed
- Shivvers SA, Wians FH Jr, Keffer JH, et al. Maternal cardiac troponin I levels during normal labor and delivery. Am J Obstet Gynecol. 1999;180(1 Pt 1):122. PubMed
- Fleming SM, O'Gorman T, Finn J, et al. Cardiac troponin I in pre-eclampsia and gestational hypertension. BJOG. 2000;107(11):1417-20. PubMed
- Abramov Y, Abramov D, Abrahamov A, et al. Elevation of serum creatine phosphokinase and its MB isoenzyme during normal labor and early puerperium. Acta Obstet Gynecol Scand. 1996;75(3):255-20. PubMed
- Afari HA, Davis EF, Sarma AA. Echocardiography for the Pregnant Heart. Curr Treat Options Cardiovasc Med. 2021;23(8):55. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.