Key Points
- Subanesthetic intravenous ketamine should be considered for patients undergoing procedures associated with severe postoperative pain, such as abdominal and thoracic surgery and orthopedic (limb and spine) procedures.
- Ketamine should be considered for opioid-dependent/tolerant patients as an adjunct therapy to limit the use of opiates when undergoing surgery or in patients with chronic medical conditions such as those with sickle cell crises.
- For chronic regional pain syndromes (CRPS), there is moderate certainty evidence supporting the use of ketamine infusions for analgesia, which has been shown to provide pain relief for up to 12 weeks.
- For chronic pain secondary to mixed neuropathic pain, fibromyalgia, cancer pain, ischemic pain, migraine headache, and low-back pain, there is weak or no evidence to support the use of ketamine infusion for immediate pain relief.
Pharmacology1-3
- Ketamine is a nonopioid, intravenous anesthetic agent that acts as a N-methyl-D-aspartate (NMDA) antagonist (Table 1).

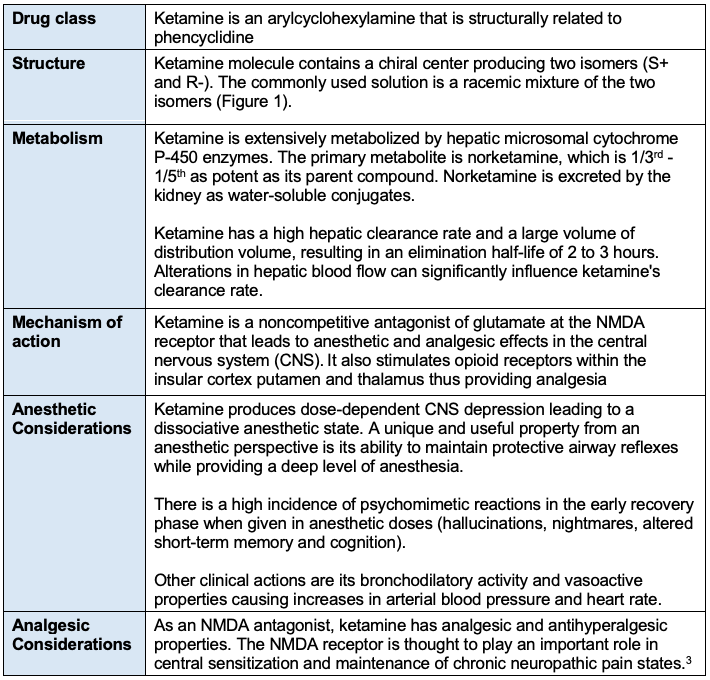
Table 1. Pharmacology of ketamine
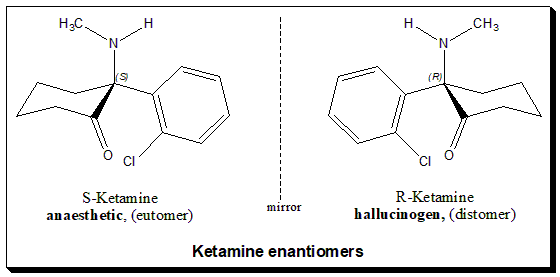
Figure 1. Ketamine enantiomers. Source: Wikimedia Commons. Valliappan Kannappan, CC BY-SA 4.0. Link.
{kind=link}
Intravenous Ketamine for Acute and Chronic Pain Management
In 2018, the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists published the following consensus guidelines for the use of ketamine for acute and chronic pain management.4,5
- Subanesthetic intravenous ketamine should be considered for patients undergoing procedures associated with severe postoperative pain, such as abdominal and thoracic surgery and orthopedic (limb and spine) procedures.
- Patients undergoing procedures that are expected to have mild pain levels do not benefit from ketamine infusion.
- Ketamine should be considered for opioid-dependent/tolerant patients as an adjunct therapy to limit the use of opiates when undergoing surgery or in patients with chronic medical conditions such as those with sickle cell crises.
- When used for perioperative analgesia, ketamine bolus dose should not exceed 0.35 mg/kg, and infusion rate should not exceed 1 mg/kg/hr in nonintensive care settings.
- Ketamine should be avoided in patients with severe or uncontrolled cardiovascular disease, severe liver disease, increased intracranial pressure, elevated intraocular pressure, pregnancy, and underlying psychiatric disease associated with psychosis.
- Evidence supporting patient-controlled analgesia (PCA) with ketamine as the sole analgesic agent postoperatively is limited.
- For chronic regional pain syndromes (CRPS), there is moderate certainty evidence supporting the use of ketamine infusions for analgesia, which has been shown to provide pain relief for up to 12 weeks.
- For chronic pain secondary to mixed neuropathic pain, fibromyalgia, cancer pain, ischemic pain, migraine headache, and low-back pain, there is weak or no evidence to support the use of ketamine infusion for immediate pain relief.
- Excluding CRPS, there is no evidence to support using ketamine for intermediate or long-term pain relief in these situations.
- There is low certainty evidence supporting oral ketamine as a follow-up therapy after ketamine infusions. Moreover, oral ketamine is associated with high abuse potential and should be cautiously prescribed.
- Follow-up therapy (after intravenous ketamine infusion) with intranasal ketamine for breakthrough pain is supported by moderate certainty evidence and can be used in the appropriate population.
References
- White PF, Romero G. Nonopioid intravenous anesthesia In: Barash PG, Cullen BF, Stoelting RK, eds. Clinical Anesthesia 5th ed. Lippincott Williams & Wilkins; 2006:334-352.
- Orhurhu VJ, Roberts JS, Ly N, et al. Ketamine in acute and chronic pain management. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Link
- Vadivelu N, Schermer E, Kodumudi V, et al. Role of ketamine for analgesia in adults and children. J Anaesthesiol Clin Pharmacol. 2016;32(3):298-306. PubMed
- Schwenk ES, Viscusi ER, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456-66. PubMed
- Cohen SP, Bhatia A, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for chronic pain from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):521-546. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.