Key Points
- Liver anatomy should be viewed both on a macroscopic level (lobes and segments), and microscopic level (lobules and acinus).
- The structural unit of the liver is the hexagonally shaped liver lobule, while the functional unit of the liver is the diamond-shaped liver acinus.
- Hepatocytes can regenerate following liver resection, trauma or ischemia/reperfusion injuries, and liver volume can be restored to normal size.
Introduction
- The liver is the largest solid organ in the body, weighing roughly 1.5 kg.1
- The liver has four lobes, further divided into eight independent segments.
- Within the liver are about 1,000,000 lobules. With a central vein and surrounded by portal triads, each lobule is where the hepatic blood inflow from arterial and portal systems mixes and communicates with hepatocytes and bile canaliculi before leaving the organ.
Relationship to Other Organs
- The liver is in the right upper quadrant (RUQ) of the abdomen (Figure 1).
- The anterior surface (diaphragmatic surface) of the liver is adjacent to the inferior surface of the right diaphragm.
- The posterior surface (visceral surface) of the liver resides over most of the stomach, right kidney, and intestines.

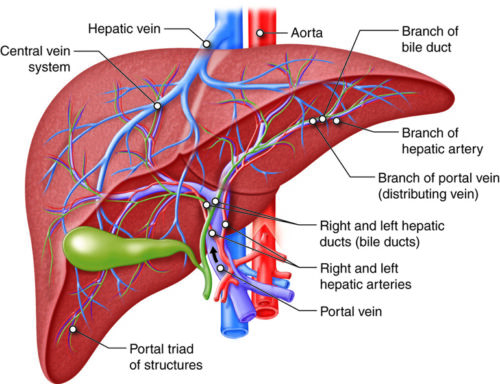
Figure 1. Basic anatomy of the liver.7
Macroscopic Anatomy
Lobes1
- There are four distinct liver lobes: right, left, caudate, and quadrate.
- The right and left lobes are visible from the anterior surface of the liver.
- The caudate and quadrate lobes are visible from the posterior surface of the liver.
- While the right lobe is anatomically the largest lobe, the left lobe is functionally the largest lobe because the quadrate lobe functions as part of the left lobe.
- The falciform ligament separates the right and left lobes.
Segments2
- The liver has 8 anatomic segments that function independently. Each segment has its own inflow, outflow, and biliary drainage (Figure 2).
- The numbering of the segments begins in a counterclockwise fashion on the posterior surface of the liver.
- Segment I: caudate lobe
- Segments II–IV: within the left lobe
- Segments V-VIII: within the right lobe
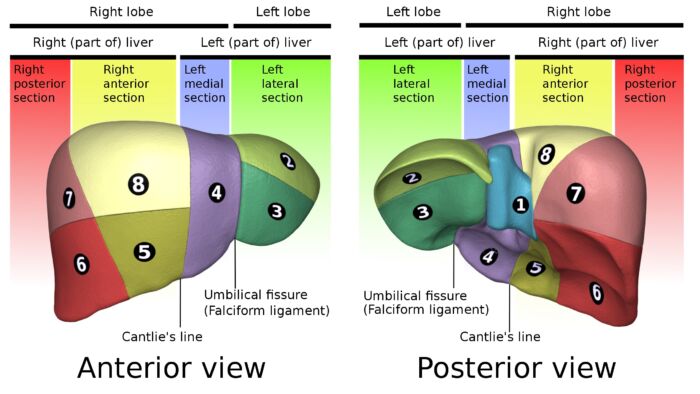
Figure 2. Couinaud classification of liver segments. From Database Center for Life Science, Wikimedia Commons CC BY-SA 2.
Extrahepatic Portal Triad
- Portal triads contain branches of the portal vein (posterolateral), hepatic artery (medial), and bile duct (lateral).
- The extrahepatic portal triad, located within the hepatoduodenal ligament, contains the main branches of the blood flow into the liver and the main biliary drainage out of the liver.
- The entry point of the extrahepatic portal triad into the liver is the porta hepatis (also enclosed in Glisson’s capsule).
Blood Supply
- The liver has a dual blood supply from the hepatic artery and the portal vein.
- Around 25% of the cardiac output goes to the liver, 75% of which is from the portal vein (PV) with the remainder from the hepatic artery (HA).
- Inflow passes though the sinusoids to the central veins, which in turn unite to form interlobular veins before exiting the liver as hepatic veins and draining into the inferior vena cava (IVC).
Microscopic Anatomy
Liver lobules1-3
- The liver lobule is the structural unit of the liver (Figure 3).
- They are characterized by the hexagonal arrangement of cords of hepatocytes which are separated by hepatic sinusoids and surround a central vein.
- Within each cord of hepatocytes are bile canaliculi.
- At the periphery of the lobules are portal triads.
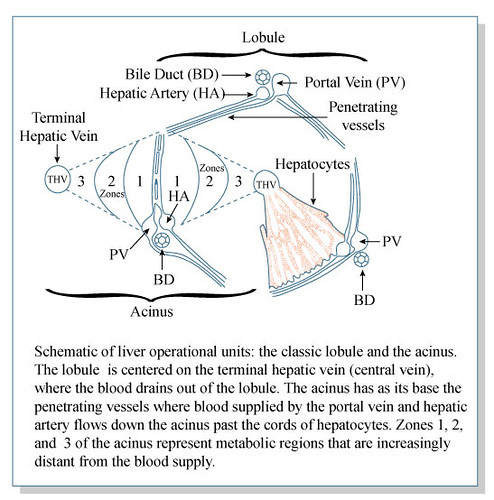
Figure 3. The operational units of the liver: lobule and acinus.8
Acinus3
- The acinus is the functional unit of the liver (Figure3).
- Unlike the lobule, which places the portal triads at the periphery, the acinus is characterized by arranging the hepatocytes in a diamond shape, placing the terminal branches of the portal triad at the center and the central veins at the two opposite corners of the diamond.
- Hepatocytes close to the portal triad (Zone 1) are exposed to oxygen-rich blood and therefore perform more oxidative tasks.
- Hepatocytes closer to the central vein (Zone 3) are exposed to oxygen-poor blood and therefore perform more metabolic functions.
- It is believed that the hepatocytes in Zone 2 have an important role in regeneration.
Intrahepatic Portal Triads
- The intrahepatic portal triads surround the liver lobules and provide end branches of portal vein, hepatic artery, and hepatic duct to the lobule.
- These vessels and ducts are the source of oxygen and metabolites for the hepatocytes, as well as the entry point of bile into the ductal system.
Sinusoids4
- The sinusoid vessels are the site of communication between the inflow, hepatocytes, bile ducts and outflow.
- Sinusoids are lined by specialized endothelial cells called liver specialized endothelial cells (LSECs). Unlike true capillary endothelial cells, which have tight junctions, the LSECs are fenestrated and lack a basement membrane. This anatomy allows for rapid transmission of hepatic blood inflow and metabolites into the sinusoids.
- LSECs have intrinsic vasodilators, the most important of which is nitric oxide (NO). When released, NO stimulates vasodilation of the hepatic sinusoids. Dilated hepatic sinusoids maintain low portal pressure within the liver.
- Low portal pressure creates a gradient for blood to easily pass from the portal circulation through to the systemic circulation.
Hepatocytes5
- The hepatocytes are arranged in a single cell plate as they surround the sinusoids.
- They project numerous microvilli into the sinusoids to increase their absorptive surface from the sinusoids.
- The average life span of a hepatocyte is 5 months. In the event of liver resections, injury and ischemia/reperfusion, hepatocytes can regenerate if the entire lobule is not destroyed, allowing the liver to return to its normal size and function.
Biliary System
- Bile canaliculi run between the hepatocytes.
- Bile enters the canaliculi and travels through a system of interlobular, septal, and major ducts within the liver, which then coalesce to form the extrahepatic bile ducts.
- The common hepatic duct joins the cystic duct to deliver bile into the intestine via the common bile duct.
References
- Trefts E, Gannon M, Wasserman DH. The liver. Curr Biol. 2017; 27(21): R1141-51. PubMed
- Sharma M, Somani P, Rameshbabu CS, et al. Stepwise evaluation of liver sectors and liver segments by endoscopic ultrasound. World J Gastrointest Endosc. 2018;10(11):326-39. PubMed
- Krishna M. Microscopic anatomy of the liver. Clin Liver Dis (Hoboken). 2013;2(Suppl 1): S4-7. PubMed
- Poisson J, Lemoinne S, Boulanger C, et al. Liver sinusoidal endothelial cells: Physiology and role in liver diseases. J Hepatol. 2017;66(1):212-227. PubMed
- Lowe JS, Anderson PG, Anderson SI. In: Stevens & Lowe's Human Histology. 5th edition. 2020. Elsevier. 209-21.
- Michaelopoulos GK. Liver regeneration. J Cell Physiol. Nov 2007; 213(2): 286-300. PubMed
- Cenveo - Drawing Liver anatomy and vascularisation - English labels. CC BY NC SA. Link
- MIT Open Course Ware. 2007. CC BY NC SA 4.0 Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.