Key Points
- Noise, music, personal reading, electronic device usage, and environmental distractions in the operating room (OR) could affect patient care.
- Certain sources of distraction, such as music, are associated with calming effects and improved focus. Others, such as unnecessary OR entries/exits, pose no clear benefits.
- Professionalism and judgment are critical in ensuring that any sources of distractions do not harm the patient. Future research is needed to clarify the objective impacts of distractions on patient outcomes.
Introduction
- In an unpredictable OR, maintaining focus is crucial to ensuring surgical and anesthetic precision and patient safety.
- However, numerous distractions to the anesthesia team, including noise, music, and personal electronic device usage, can negatively affect patient outcomes.
- This summary examines current research to determine the subjective and objective impacts of distractions on the healthcare personnel in the OR and, ultimately, the patient.
Noise and Music
Noise in the OR
- Noise in the OR is a significant concern for surgical performance and staff well-being.
- High noise levels have been associated with decreased mental efficiency, short-term memory, and increased workload among anesthesia residents.1
- The U.S. Environmental Protection Agency recommends noise levels below 75 dB over 8 hours to prevent hearing loss and less than 45 dB indoors to prevent task interference.1
- One study showed that OR noise levels averaged 71.9 dB during critical phases such as induction and emergence.1
- Common noise sources in the OR are shown in Table 1.

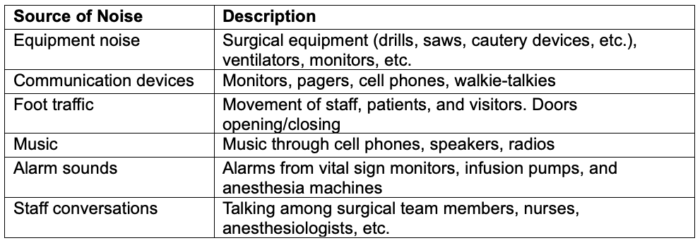
Table 1. Common sources of noise in the OR. Adapted from Gui JL, Nemergut EC, Forkin KT. J Clinical Anesth. 2021.1
- Interventions to reduce OR noise, such as education and reminders, have effectively decreased overall noise distractions.1
- In addition to monitoring noise levels, specific strategies like the “sterile cockpit” (only allowing the presence of essential staff in the OR during induction and emergence) have been suggested.1
- Another promising solution is implementing a “plan-do-study-act” model to implement noise and distraction-reducing interventions.2
- One study that implemented several interventions in this manner (circulating nurse pausing music before patient enters the OR, anesthesiologist ensuring quiet OR during induction, and educating perioperative, anesthesia, and surgical staff) reduced the percentage of cases with a distraction during induction from 61% to 10% within five months.2
- Minimizing noise may benefit patient safety during sensitive procedures such as induction/emergence or neonatal delivery during cesarean deliveries.1
Music in the OR
- Seventy-two point two percent (72.2%) of anesthesiologists report the regular presence of music in the OR.1
- Anesthesia providers often find music distracting (51%), that it reduces vigilance (26%), that it and impairs communication (24%) during critical situations.1
- While some studies suggest music’s benefits, its impact on surgical performance in nonsimulated ORs remains unclear.3
- Most OR personnel agree that music should be allowed in the OR, aiding focus (63%) and calming effects (75%).3
- Volume was noted as the primary distractor (73%), followed by genre (10%) and lyrics (5%).3
- The pros and cons of music in the OR are shown in Table 2.
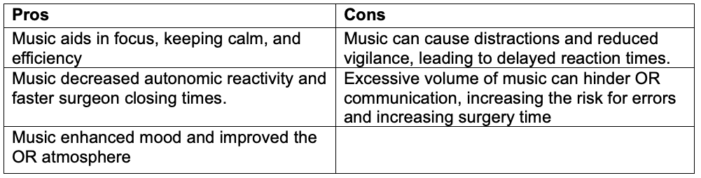
Table 2. Pros and cons of music in the OR. Adapted from Lamberton T, et al. Am Surgeon. 2022.3
- Overall, a joint decision regarding music volume and genre is recommended to ensure focus and patient safety.3
- Despite these challenges, the benefits of music in reducing stress and improving focus cannot be ignored. Further research and collaborative decision-making processes are needed within the OR environment.
Personal Distractions
Personal Electronic Device Use
- Personal electronic devices (PEDs) are commonly used in the OR.
- A Turkish survey of 955 anesthesia providers revealed that 93.7% use smartphones during patient care, including usage for calls (65.4%), messaging (46.4%), social media (35.3%), and internet (33.7%).4
- However, 96.7% of respondents reported that they never used PEDs during critical anesthesia stages, and 87.3% stated that they were never distracted by PEDs. Despite this, 41% witnessed a fellow provider being distracted by PEDs at least once.4
- Another survey utilized a modified CAGE questionnaire to assess a risk/benefit analysis of PED usage by anesthesiologists, residents, and CRNAs.5
- Felt the need to Cut down on PED usage
- Annoyed by others for using PEDs
- Guilt about using PEDs
- Reaching for PED as soon as waking up (Eye-opener)
- Out of 647 respondents, 21% had a positive CAGE screen (agreed to at least two out of the four CAGE questions), indicating potentially addictive and distracting behaviors related to PED usage.5
- However, nearly all respondents felt that the benefits of OR PED usage, including the rapid availability of medical information, at least somewhat outweigh the risks.5
- One proposed solution is routine training on situational awareness and the dangers of multitasking.5
- Further research is needed to understand the risks of PED use in ORs.
Intraoperative Activities
- Intraoperative reading (diverting attention away from a case to perform another work or personal task) is common among anesthesia providers, particularly during periods of low workload.1
- One study found intraoperative reading occurred in 34.9% of cases, mainly during the maintenance phase of anesthesia.1,6
- Vigilance latency, as measured by the response time to a light indicator, was not different among those participating in intraoperative reading vs. not.1,6
- Anesthesia providers spent less time conversing with others while reading.1
- The most common forms of intraoperative reading included internet use (50.7%) and email use (25.4%).1
- There is no direct evidence suggesting intraoperative reading jeopardizes patient safety. However, professionalism and sound clinical judgment are vital, especially during intense periods and for less experienced providers.1,6
- More research on nonrecord-keeping activities during patient care is needed to assess impacts on patient outcomes.
Other Environmental Distractions
- Research shows equipment-related distractions are more intense and longer-lasting than other common distractions, such as small talk or intraoperative teaching.1
- One study showed that workspace and equipment-related distractions accounted for 21.5% and 10.8% of all distracting events, respectively, while observing 30 anesthesia cases.1
- Staff entering/exiting the OR is another major distraction, particularly during critical moments like establishing neuraxial blockade.1
- Hospitals should prioritize well-designed workspaces and ensure adequate equipment to minimize distractions.1
- OR staff should be educated to minimize unnecessary entries/exits and maintain a quiet environment during surgeries.1
Summary
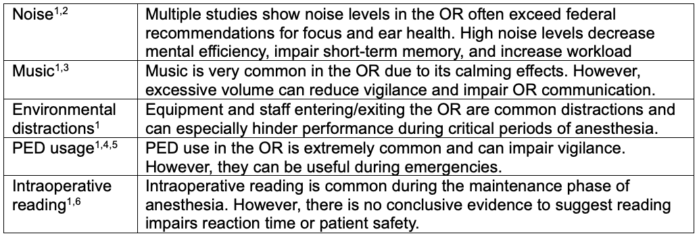
Table 3. Summary of OR distractions
References
- Gui JL, Nemergut EC, Forkin KT. Distraction in the operating room: A narrative review of environmental and self-initiated distractions and their effect on anesthesia providers. J Clinical Anesth. 2021; 68:110110. PubMed
- Crockett CJ, Donahue BS, Vandivier DC. Distraction-free induction zone: A Quality Improvement Initiative at a large academic children’s hospital to improve the quality and safety of anesthetic care for our patients. Anesth Analg. 2019;129(3):794-803. PubMed
- Lamberton T, de Virgilio C, Terrell J, et al. Music in the operating room: Comparing the opinions of surgeons, anesthesiologists, and nurses. Am Surgeon. 2022;89(12):5234-9. PubMed
- Pınar HU, Karaca O, Doğan R, Konuk ÜM. Smartphone use habits of anesthesia providers during Anesthetized Patient Care: A survey from Turkey. BMC Anesthesiology. 2015;16(1). PubMed
- Soto RG, Neves SE, Papadakos PJ, Shapiro FE. Personal electronic device use in the operating room. Eur J Anaesthesiol. 2017;34(4):246-7. PubMed
- Slagle JM, Weinger MB. Effects of intraoperative reading on vigilance and workload during anesthesia care in an Academic Medical Center. Anesthesiology. 2009;110(2):275-83. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.