Key Points
- CHARGE syndrome is a rare genetic disorder characterized by coloboma, choanal atresia, and hearing abnormalities.
- Airway management can be challenging due to micrognathia, laryngomalacia, choanal atresia, and possible tracheoesophageal fistula.
- Patients are at elevated risk of postoperative adverse airway events.
- Perioperative communication may be challenging as most patients have visual and hearing loss.
Introduction
- The group of anomalies was first described in 1979 in patients with choanal atresia and other abnormalities.1
- In 1981, the term “CHARGE association” was described using some of the features for the acronym Coloboma, Heart defect, Atresia choanae, Retarded growth, Genital hypoplasia, and Ear hypoplasia or deafness.2,3
- The term “CHARGE syndrome” is used currently since most patients have been identified to have mutations within the CHD7 gene on chromosome 8q12.2,3
- The incidence of CHARGE syndrome is estimated to range from 0.1-1.2/10,000 live births.2
- Most cases are due to de novo mutations in the CHD7 gene that occur sporadically.2,3
- Autosomal dominant inheritance with variable expressivity has also been reported.
- A clinical diagnosis of typical CHARGE syndrome is when patients have three major criteria or two major and two minor criteria (Table 1).3

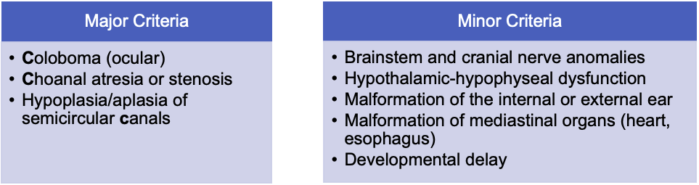
Table 1. Updated clinical criteria for the diagnosis of CHARGE syndrome.3
Clinical Presentation and Associated Anomalies
There is wide variation in the presentation of patients with CHARGE syndrome.
Colobomas2,3
- Colobomas and other eye abnormalities are reported in the majority (75-90%) of patients.2,3
- Colobomas are usually bilateral, and involve the eye lid, iris, retina, choroid, optic disc, or macula. The typical coloboma is chorioretinal and predisposes to retinal detachment and visual impairment (Figure 1).
- Vision may be normal or severely impaired.

Figure 1. Coloboma of the iris. Source: Wikipedia. Jmarchn. CC BY-SA 3.0
Heart Defects2,3
- They occur in 75-80% of patients with CHARGE syndrome.
- Conotruncal heart defects (tetralogy of Fallot, double-outlet right ventricle, interrupted aortic arch) and atrioventricular septal defects are common.
Choanal Atresia/Airway anomalies2,3
- Choanal atresia is present in about 65% of patients.
- It may be unilateral or bilateral and can be membranous or bony.
- Bilateral choanal atresia presents at birth with respiratory distress or cyanosis as infants are obligate nasal breathers. Symptoms improve with crying.
- Airway obstruction is present in about 70% of patients: laryngomalacia (40%), tracheomalacia (20%), and subglottic stenosis (10%).
- Cleft lip and palate are seen in about 15-20% of patients.
- Tracheoesophageal fistula is seen in about 15-20% of patients.
- Obstructive sleep apnea is present in about 65% of patients.4
Growth and Developmental Retardation2,3
- Growth retardation results in short stature and pubertal delay.
- Cognitive impairment is common with low intelligence quotient that is less than 70 in over 70% of patients. This often results in communication and language delay.
Genitourinary Problems2,3
- Genital hypoplasia is common with cryptorchidism and micropenis in males and hypoplastic labia and clitoris in females.
- Delayed puberty or pubertal arrest is common.
Ear and Hearing Problems2,3
- Ear anomalies are reported in 85-100% of patients.
- The characteristic external ear appearance is a wide, low set, and cup-shaped ear with a hypoplastic lobule. A triangular concha is a common finding (Figure 2).
- The most common inner ear abnormality is the absence of the lateral semicircular canals.
- Both conductive and sensorineural hearing loss is common.

Figure 2. Patient with CHARGE syndrome and characteristic ear shape. Blake KD, Prasad C. CHARGE syndrome. Orphanet J Rare Dis. 2006; 1:34.2 CC BY 2.0.
Cranial Nerve Anomalies
- Cranial nerve (CN) dysfunctions include the CN I (anosmia in almost all patients), CN VII (facial palsy), CN VIII (sensorineural hearing loss), and CN IX/X/XI (feeding and swallowing issues, velopharyngeal insufficiency).
- Conditions with similar or overlapping elements include VACTERL association, 22q11 deletion syndrome, and oculo-auriculo-vertebral spectrum.2,3
Preanesthetic Evaluation
- Many features of CHARGE require anesthesia for diagnostic or surgical interventions during childhood.
- Most patients will require surgery within the first two months of life.5
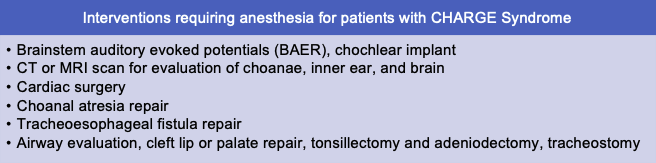
Table 2. Common diagnostic and surgical interventions for patients with CHARGE syndrome.
- A multidisciplinary consultation with general pediatrics, medical genetics, otolaryngology, cardiology, and ophthalmology should be considered to guide evaluation.3
- History
- Prior surgeries, anesthetics, and intubations
- Developmental stage, coping skills, cooperation (if considering awake intubation)
- Physical exam
- Perform detailed airway evaluation
- Evaluate for lower respiratory signs of chronic aspiration or pneumonia
- Evaluate for cardiac murmurs
- Imaging
- Echocardiogram
Anesthetic Considerations and Management
- Anticipate challenges with communication and cooperation and consider premedication (Table 3).
- Subacute bacterial endocarditis prophylaxis may be indicated.
- An increased risk of aspiration due to reflux and secretion intolerance may be present.
- Micrognathia increases the risk of difficulty with intubation.6
- Laryngomalacia places CHARGE patients at an increased risk of obstruction due to upper airway collapse during anesthesia.6 Patients may require increased positive end-expiratory pressure with mask ventilation or when using a supraglottic airway.
- Postoperative adverse airway events are common in patients with CHARGE syndrome.5
- Consider combining procedures under a single anesthetic.
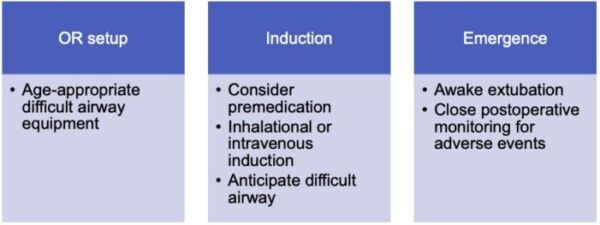
Table 3. Summary of anesthesia setup and management for patients with CHARGE syndrome.
Emergence
- Neuromuscular blockade should be reversed.
- Secretions should be carefully suctioned given swallowing dysfunction.
- Close monitoring should be ensured during recovery from anesthesia due to risks of airway events.
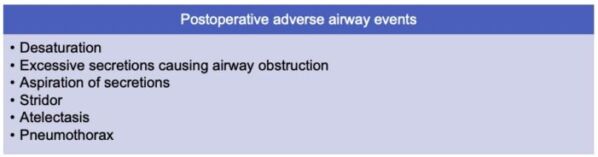
Table 4. Post operative adverse airway events in patients with CHARGE syndrome. Adapted from Blake K, et al. Postoperative airway events of individuals with CHARGE syndrome. Int J Pediatr Otorhinolaryngol. 2009;73(2):219-26.5
References
- Hall BD. Choanal atresia and associated multiple anomalies. J Pediatr. 1979;95(3): 395-8. PubMed
- Blake KD, Prasad C. CHARGE syndrome. Orphanet J Rare Dis. 2006:1:34. PubMed
- Hsu P, Ma A, Wilson M, et al. CHARGE syndrome: a review. J Paediatr Child Health. 2014;50(7): 504-11. PubMed
- Trider CL, Corsten G, Morrison D, et al. Understanding obstructive sleep apnea in children with CHARGE syndrome. Int J Pediatric Otorhinolaryngol. 2012;76(7): 947-53. PubMed
- Blake K, MacCuspie J, Hartshorne TS, et al. Postoperative airway events of individuals with CHARGE syndrome. Int J Pediatr Otorhinolaryngol. 2009;73(2): 219-26. PubMed
- Stack CG, Wyse RK. Incidence and management of airway problems in the CHARGE association. Anaesthesia. 1991;46(7): 582-85. PubMed
Other References
- Usman N, Moushumi S. CHARGE Syndrome In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. 2022 May 11. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.