Key Points
- Alpha blockers lower blood pressure by antagonizing alpha-adrenergic receptors, particularly alpha-1 receptors on vascular smooth muscle, leading to vasodilation and decreased systemic vascular resistance.
- Orthostatic hypotension is a possible side effect and can be serious in vulnerable populations, such as the elderly.
- Common clinical uses of alpha blockers include treatment of hypertension and benign prostatic hyperplasia (BPH) (alpha-1 blockers), preoperative management of pheochromocytoma (nonselective alpha blockers).
Introduction
- Alpha-adrenergic antagonists are primarily used to manage essential hypertension, BPH, and pheochromocytoma.1
- Alpha-adrenergic antagonists inhibit the sympathetic nervous system activity by blocking alpha-1 receptors, leading to vasodilation and a reduction in blood pressure.1
- Selective alpha-1 blockers are preferred for BPH and hypertension due to fewer side effects than nonselective alpha blockers, while nonselective alpha blockers are used perioperatively in pheochromocytoma.1
- A significant side effect is orthostatic hypotension, which can affect perioperative stability.1
Mechanism of Action
- There are two known alpha receptors: alpha-1 and alpha-2.
- Alpha-1 receptors are found mostly in vascular smooth muscle, bladder neck and prostate, pupillary dilator muscle, liver, and intestinal smooth muscle. Binding to alpha-1 receptors results in vasoconstriction and subsequently increased blood pressure.2
- Alpha-2 receptors are found mostly in presynaptic nerve terminals, platelets, pancreatic islet cells, and vascular smooth muscle. Binding to alpha-2 receptors inhibits sympathetic signals via presynaptic feedback inhibition, thus lowering vascular tone and blood pressure.2
- Alpha-1 and alpha-2 receptors act through different signalling cascades:
- Alpha-1 receptors are Gq coupled, and when activated, lead to activation of phospholipase C, leading to increases in inositol triphosphate and diacylglycerol, ultimately leading to increased intracellular calcium.2
- Alpha-2 receptors are Gi coupled, and when activated, lead to inhibition of adenylyl cyclase, which decreases the formation of intracellular cyclic adenosine monophosphate.2
- Alpha blockers inhibit the effects of endogenous catecholamines, such as norepinephrine (NE), at alpha-adrenergic receptors. While alpha-1 antagonism leads to vasodilation and decreased systemic vascular resistance, alpha-2 antagonism can increase NE release by blocking presynaptic feedback inhibition, potentially heightening sympathetic tone.2

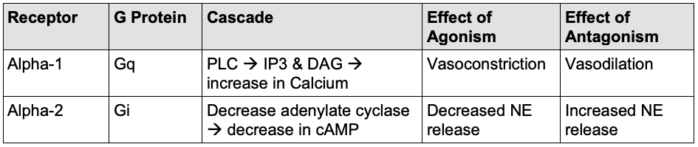
Table 1. Summary of alpha receptor cascade and blocker effect. Abbreviations: PLC, phospholipase C; IP3, inositol triphosphate; DAG, diacylglycerol; cAMP, cyclic adenosine monophosphate; NE, norepinephrine.
Pharmacokinetic
- The majority of alpha blockers are metabolized by the liver and excreted through bile and the kidneys.3
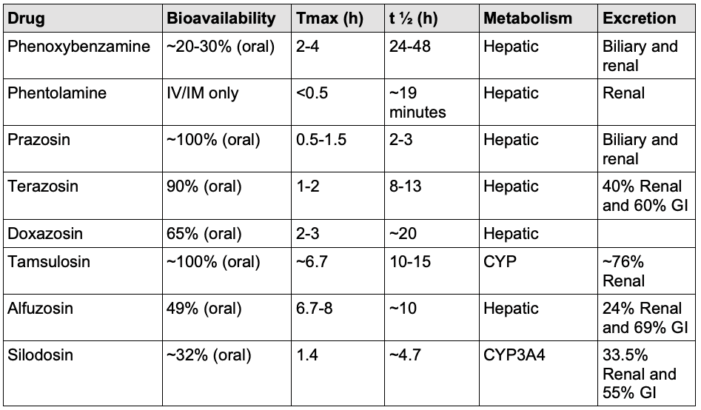
Table 2. Pharmacokinetic properties of common alpha blockers. Abbreviations: GI, gastrointestinal.3,6,7,8
Systemic Effects
- Nonselective alpha antagonists cause vasodilation, leading to decreased systemic vascular resistance and blood pressure, which can result in orthostatic hypotension due to impaired vasoconstriction.2 Reflex tachycardia results due to baroreceptor-mediated increased sympathetic tone.2 Additional systemic effects include nasal congestion, miosis, increased gastrointestinal motility, and inhibition of ejaculation.2
- Selective alpha-1 antagonists lower blood pressure through vasodilation, which can result in orthostatic hypotension, and result in mild reflex tachycardia.2 They also improve urinary flow in BPH by relaxing smooth muscle in the bladder neck and prostate. They can also cause nasal congestion.2
- Selective alpha-2 antagonists increase sympathetic outflow through increased NE release, which leads to elevated heart rate and blood pressure, along with potential central nervous system stimulation (anxiety and agitation), and increased insulin secretion.2 Selective alpha-2 antagonists have a limited role in clinical medicine, though the tetracyclic antidepressant mirtazapine does antagonize alpha-2 receptors in addition to other mechanisms of action.
Clinical Uses
- Nonselective alpha blockers (phenoxybenzamine and phentolamine) and selective alpha-1 antagonists are approved for the management of pheochromocytoma, a catecholamine-secreting tumor, to prevent hypertensive crises.1
- Nonselective blockade is associated with less intraoperative hypertension.4
- Alpha blockers are administered preoperatively (titrated up over 7 days prior to surgery) to counteract excess catecholamine secretion and stabilize intraoperative hemodynamics.4 The Roizen criteria are used to assess the adequacy of alpha blockade before surgery.5
- Beta blockade should only be initiated after alpha blockade has been established. Isolated beta blockade in a patient with pheochromocytoma can precipitate hypertensive crisis by displacement of catechols from beta receptors onto unantagonized alpha receptors.5
- Please see the OA summary on pheochromocytoma for more details. Link
- In the perioperative setting beyond pheochromocytoma, nonselective alpha antagonists, specifically phentolamine, can be used to manage hypertensive crises (such as that caused by cocaine toxicity, e.g.) more broadly.1,4,5
- Phentolamine is also used for reversing intense vasoconstriction caused by extravasated vasopressors.1
- Selective alpha-1 blockers are FDA-approved for the treatment of BPH and hypertension.1 They are also second-line agents for essential hypertension.1
- Common indications of alpha blockers are listed in Table 1.
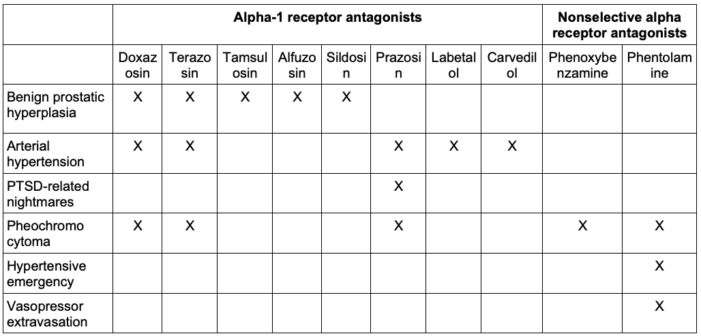
Table 3. Common indications for alpha blockers.1,4,5
- Additionally, there are a variety of agents with alpha-adrenergic blocking properties but whose major clinical use appears to be unrelated: mirtazapine, haloperidol, fluphenazine, chlorpromazine, thioridazine, quinidine, bromocriptine, amiodarone, verapamil, and ketaserin.6
Dosage
- Phenoxybenzamine is a long-acting oral medication used most often preoperatively for pheochromocytoma.
- Dosing is started at least 7 days before surgery, but often 10 to 14 days prior. Initial dosing is 10 mg twice.1 Dose can be increased every other day, usually reaching 20-40 mg two or three times daily.1
- Phentolamine is often used as an adjunct to control blood pressure before and during the removal of pheochromocytoma.1 Typical dose is 5 mg administered intramuscularly or intravenously.1
- Selective alpha-1 blockers are often dosed at nighttime to reduce the risk of orthostatic hypotension.1 Elderly patients should initially receive a halved dose.1
- The standard dose of tamsulosin is 0.4 mg once daily.1,8 It may be increased to 0.8 mg for those who fail to respond to a lower dose.8
- Alfuzosin should be taken with meals and is a 10 mg once daily dose for BPH.8 Dosage adjustment should be practiced for patients with renal and/or hepatic impairment.8
- The starting dosage of doxazosin is 1 mg orally.8 The maximum dose for targeting hypertension is 16 mg/day; for BPH, it is 8 mg/day.8
- The starting dose of prazosin is 1 mg two to three times per day.8 Maintenance dose is 3-15 mg/day divided into 2-4 times/day.8 Maximum dosage is 20 mg daily.8 To target hypertensive urgency, a 10-20 mg dose is given once and may be repeated every thirty minutes.8
- Silodosin is administered orally in 8 mg capsules once daily. In those with renal impairment, the dose is 4 mg.8
- The starting dose of terazosin is 1 mg. It may be titrated to 20 mg/day to achieve the desired blood pressure.8
Side Effects/Toxicity
- Side effects tend to be highly dose-dependent.1,3
- Nonselective alpha blockers can cause hypotension by inhibiting alpha-1 receptors, leading to relaxation of vascular smooth muscle and vasodilation. Sudden drops in blood pressure can result in reflex tachycardia. There is a particular risk of hypotension with spinal anesthesia in patients who are using nonselective and alpha-1 blockers.
- Patients with alpha-1 blockers are at an increased risk of intraoperative floppy iris syndrome during eye procedures.1
- Alpha-2 blockade results in increased NE release, which often stimulates beta receptors, resulting in tremors and tachycardia.
- Additional side effects from alpha-1 blockers include headaches, weakness, nausea, and sexual dysfunction, including retrograde ejaculation or impotence, but these are rare.3
Contraindications
- Alpha blockers should be used with caution in patients with a history of orthostatic hypotension and in elderly patients due to the potential increased risk of falls.1,7
- Alpha blockers should be avoided in those undergoing cataract surgery due to the risk of intraoperative floppy iris syndrome – a phenomenon caused by atrophy of the iris dilator muscle.1
- Phenoxybenzamine and phentolamine are contraindicated in breastfeeding mothers due to the potential risks of fetal cardiovascular malformation and intrauterine growth restriction.1
References
- Nachawati D, Leslie SW, Patel JB. Alpha-Blockers. In: StatPearls (Internet). Treasure Island, FL. StatPearls Publishing; 2025. Accessed June 10, 2025. StatPearls Link
- Nash DT. Alpha-adrenergic blockers: Mechanism of action, blood pressure control, and effects on lipoprotein metabolism. Clin Cardiol. 1990; 13 (11): 764-772. PubMed
- Donnelly R, Merredith P, Elliott HL. Pharmacokinetic-pharmacodynamic relationships of alpha-adrenoceptor antagonists. Clin Pharmacokinet. 1989; 17 (4): 264-274. PubMed
- Kong H, Li N, Yang X, et al. Nonselective compared with selective alpha-blockade is associated with less intraoperative hypertension in patients with pheochromocytomas and paragangliomas: A retrospective cohort study with propensity score matching. Anesth Analg. 2021; 132 (1): 140-149. PubMed
- Naranjo J, Dodd S, Martin YN. Perioperative management of pheochromocytoma. J Cardiothorac Vasc Anesth. 2017; 31(4):1427-1439. PubMed
- Sica D. Alpha1-Adrenergic blockers: Current usage considerations. J Clin Hypertens. 2007; 7 (13): 757-762. PubMed
- Frishman W, Kotob F. Alpha-adrenergic blocking drugs in clinical medicine. J Clin Pharmacol. 1999; 39 (1): 7-16. PubMed
- McAuley D. Alpha blockers. Global RPH. 2017. Accessed June 21, 2025. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.