Key Points
- Emergency airway management (EAM) has a significant complication rate when performed outside the operating room.
- A team-based multidisciplinary approach is ideal for emergency airway management.
- Implementing an airway response team (ART) may help reduce morbidity, mortality, and significant complication rates in patients requiring EAM.
Challenges of Emergency Airway Management1
- Critically ill patients in the hospital frequently require EAM. Despite advances in airway management and technology, the complication rate from EAM outside the operating room exceeds 45%.1
- Adverse events surrounding EAM are often multifactorial, including inconsistent communication among hospital staff, lack of defined roles during events, and provider unfamiliarity with techniques and equipment.
- Possible complications include hypoxemia leading to hypoxic brain injury, hypercarbia, alterations in blood pressure, temporomandibular joint dislocation, cervical spine injury, aspiration, laryngospasm, esophageal or mainstem bronchus intubation, and injury to teeth, soft tissue, and vocal cords.
- Unplanned intubations lead to various challenges in settings outside of the operating room. Patient-related, procedure-related, and environment-related challenges are summarized in Table 1.

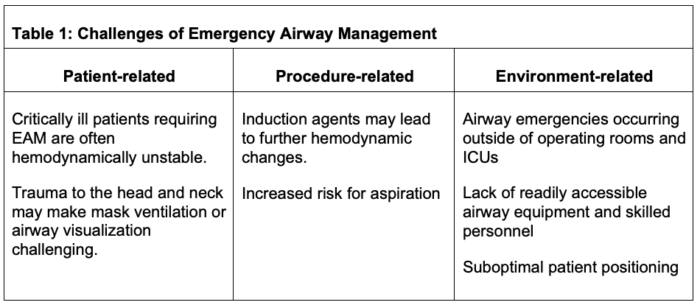
Table 1. Summary of the challenges of emergency airway management. Adapted from Tankard KA, et al. Design and Implementation of airway response teams to improve the practice of emergency airway management. J Clin Med. 2022;11(21):6336. CC BY 4.0.
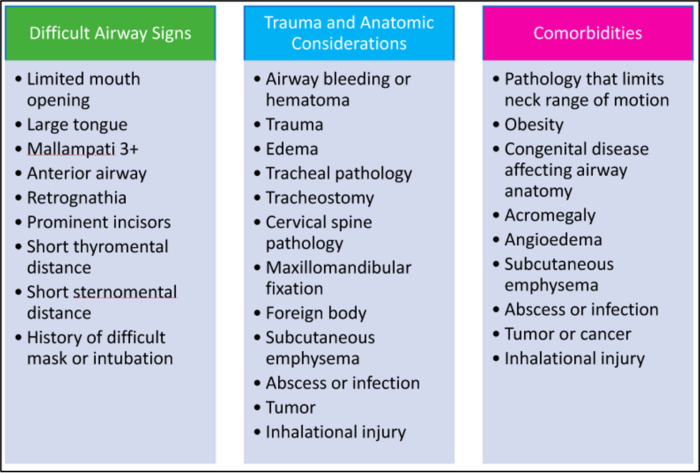
Table 2. Patient characteristics and factors indicative of a difficult airway. From Tankard KA, et al. Design and Implementation of airway response teams to improve the practice of emergency airway management. J Clin Med. 2022;11(21):6336. CC BY 4.0.
The Airway Response Team (ART) Model1,2
- Growing evidence suggests that implementing an ART model may help reduce morbidity, mortality, and significant complication rates in patients requiring EAM.
- The ART ideally consists of two clinicians with difficult airway experience: an anesthesiologist and a surgeon trained in performing surgical airways. It may be challenging for smaller community or rural hospitals to initiate continuous coverage. Based on resources, a range of physicians, including emergency medicine physicians and intensivists, could be used. The team may also include a respiratory therapist, pharmacist, nurse, and equipment technician. During an emergency airway event, team members should have defined roles in place (Figure 1).
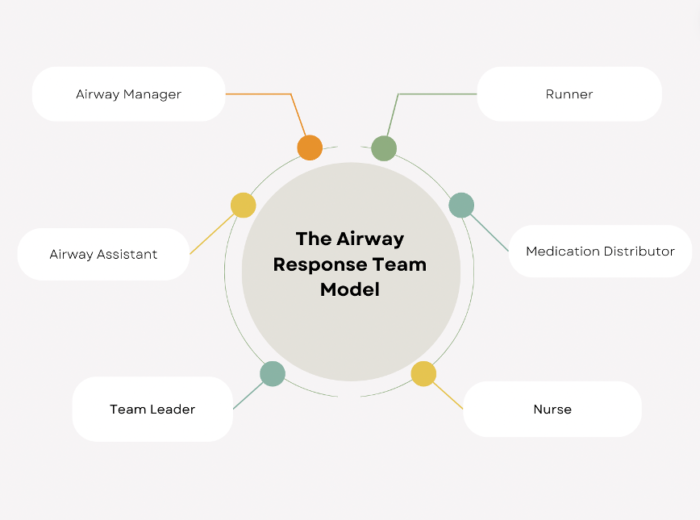
Figure 1. The Airway Response Team Model
- An essential component of the ART model is easy access to a defined set of emergency airway equipment tools. One possible intervention is placing difficult airway carts in various areas of the hospital, including each ICU, emergency room, obstetrics unit, and operating room area. Each cart should be identical in appearance and stocked with equipment that is organized, easy to use, and reliably restocked. Carts may consist of the following tools: disposable laryngoscope and bronchoscopy system with dual view capability so two clinicians can work simultaneously, fiberoptic and rigid bronchoscopy equipment, and equipment for cricothyrotomy and tracheostomy. Images of an example difficult airway cart (Figure 2) and cart inventory list (Table 3) are shown below.
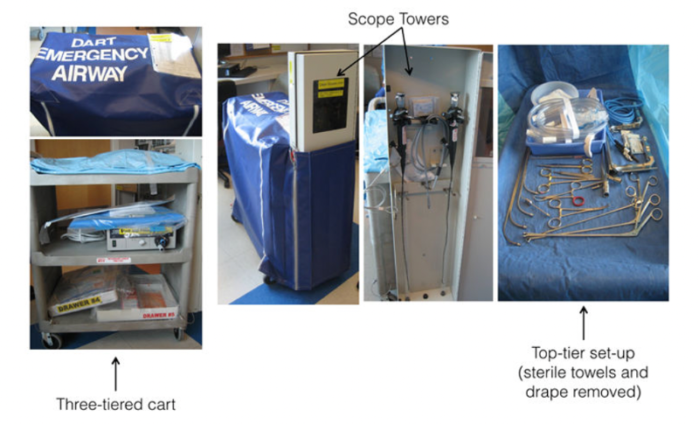
Figure 2. Airway response team (ART) three-tiered cart containing various instruments, bronchoscopes, and a top-tier set-up. Used with permission from Mark LJ, et al. Difficult airway response team: a novel quality improvement program for managing hospital-wide airway emergencies. Anesth Analg. 2015;121(1):127-139.
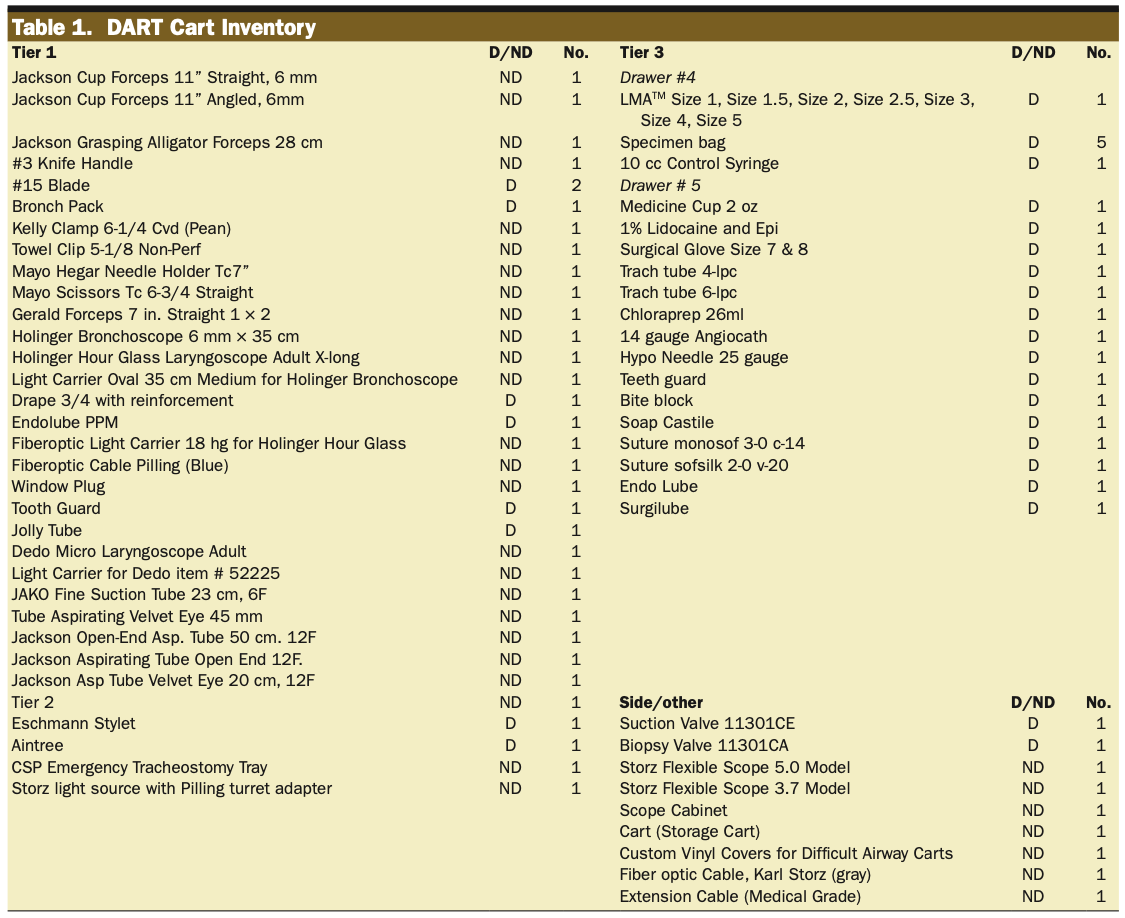
Table 3. Airway response team (ART) cart inventory. Abbreviations: D= disposable; ND = non-disposable. Used with permission from Mark LJ, et al. Difficult airway response team: a novel quality improvement program for managing hospital-wide airway emergencies. Anesth Analg. 2015;121(1):127-139.
Considerations for Implementation3
- Creating an ART requires collaboration and support from clinicians and hospital leadership. Before initiating an ART model, a thorough assessment of current airway protocols and equipment should be conducted.
- The ART includes a clear activation or paging process and prompt response. Hospital staff should be educated on when and how to activate the ART. To protect patient safety, the ART must ensure 24-hour availability.
- Early identification of patients with risks of a difficult airway is important. Patients at high risk for a difficult airway can be identified by a difficult airway wristband, posters above the patient’s hospital bed, and/or designation in the EMR.
- Airway response team members should be trained using real-life scenarios and simulation-based exercises. Airway workshops, monthly reviews of difficult cases, and quality improvement surveys may help reduce negative outcomes and improve team member competency.
- Possible barriers to implementation include the availability and cost of airway equipment, team member scheduling conflicts, and potential time and resources needed to educate the ART members and other hospital staff.
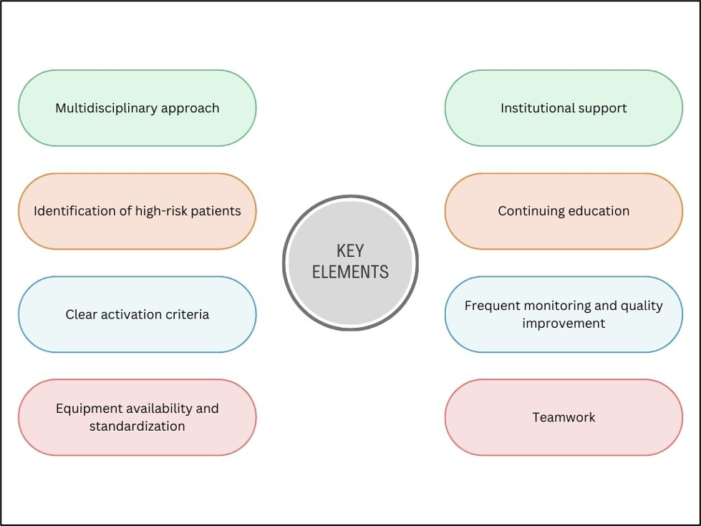
Figure 3. Key elements for effective airway response teams. Adapted from Tankard KA, et al. Design and implementation of airway response teams to improve the practice of emergency airway management. J Clin Med. 2022;11(21):6336. CC BY 4.0.
References
- Tankard KA, Sharifpour M, Chang MG, Bittner EA. Design and implementation of airway response teams to improve the practice of emergency airway management. J Clin Med. 2022;11(21):6336. PubMed
- Atkins JH, Rassekh CH. Multidisciplinary airway response teams: Concept, structure, & implementation. Operative Techniques in Otolaryngology-Head and Neck Surgery. 2020;31(2):105-110. Link
- Mark LJ, Herzer KR, Cover R, et al. Difficult airway response team: a novel quality improvement program for managing hospital-wide airway emergencies. Anesth Analg. 2015;121(1):127-139. PubMed
Other References
- Bechtel A. Episode #72 Building a Difficult Airway Response Team Program. Anesthesia Patient Safety Podcast. 2021. Link
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.