Digoxin acts as an anti-arrhythmic and inotrope through reversible inhibition of cardiac Na/K ATPase pumps. This results in increased intracellular sodium and calcium and decreased intracellular potassium. Digoxin can be used for congestive heart failure as well as supraventricular tachyrhythmias but its narrow therapeutic window significantly limits its use. Digoxin toxicity can cause CNS, ocular, gastrointestinal and cardiac dysfunction. Hypokalemia potentiates the effects of digoxin. Many drugs commonly used in anesthesia can exacerbate electrolyte distubances thereby increasing risk of cardiac toxicity. Commonly implicated agents include succinylcholine, intravenous calcium, loop diuretics (furosemide) and sympathomemtics such as ephedrine.
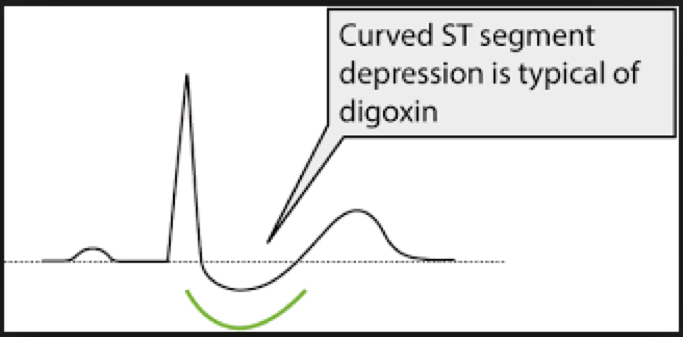
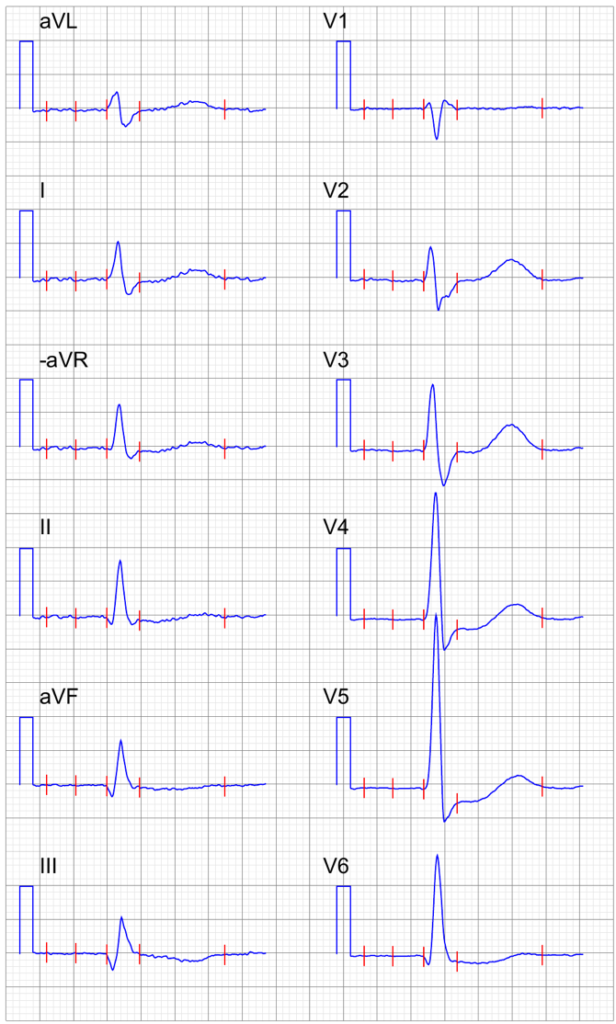
On ECG, Digoxin use will typically cause a 1st degree AV block (PR interval >240msec) and is classically associated with “reverse tick sign” or concave ST depressions.
Digoxin toxicity can cause a variety of ECG changes and virtually any arrhythmia with the exception of atrial tachycardia with RVR. Younger patients without significant heart disease are more likely to develop bradyarrhythmias whereas elderly patients and patients with severe myocardial dysfunction are more prone to developing ventricular dysrhythmias and atrial ectopy. Toxicity can result in progression of the 1st degree AV block to 2nd or 3rd degree AV block. The degree of blockade is potentiated by concomitant use of beta-blockers and calcium channel blocking agents. Classically, patients will develop a tachyarrhythmia in combination with SA or AV node suppression, such as atrial and junctional tachycardia with AV block.
Ventricular tachycardia and ventricular fibrillation can also be seen. Bidirectional ventricular tachycardia is also a possible ECG finding associated with severe digoxin toxicity.

From the (medical) gallery of Mikael Häggström, M.D.. Last updated: 2018-05-10. Licensing (unless other license is given for image): Creative Commons CC0 1.0 Universal Public Domain Dedication, used with permission.
From the (medical) gallery of Mikael Häggström, M.D.. Last updated: 2018-05-10. Licensing (unless other license is given for image): Creative Commons CC0 1.0 Universal Public Domain Dedication, used with permission.
References
- Pincus M. Management of digoxin toxicity. Aust Prescr. 2016 Feb; 39(1): 18–20. PubMed Link
Other References
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.