The Left Ventricle (LV) is a conical shaped chamber that can easily be visualized with TEE. The apex is the point of the cone and the base represents the LV inflow tract via the mitral valve and the LVOT via the Aortic Valve. Since the LV is a 3D structure, viewing it with 2D TEE requires recreating the structure in your brain to assess the whole structure. A single image of the LV doesn’t necessarily represent a complete view of LV or associated valvular function.

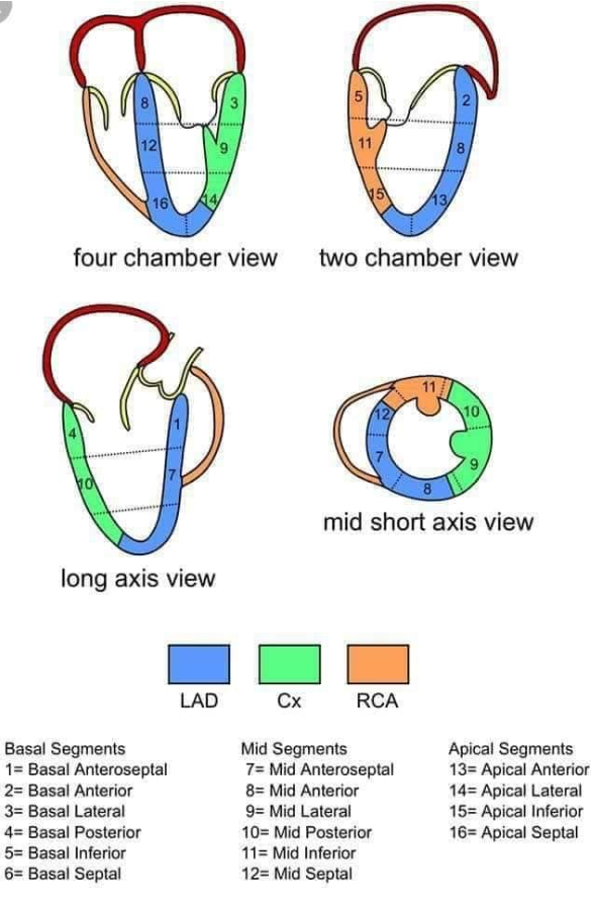
https://commons.wikimedia.org/wiki/File:TEE_coronary_region_(CardioNetworks_ECHOpedia).svg
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.