Key Points
- Porphyrias are a group of rare hereditary diseases that result in decreased activity of heme and accumulation of neurovisceral toxins.
- Acute intermittent porphyria (AIP) is the most common type and presents with abdominal pain, peripheral neuropathies, hypertension, tachyarrhythmias, and can progress to respiratory arrest.
- Both general and regional/neuraxial anesthesia have been safely administered. Drugs to avoid include barbiturates, diazepam, etomidate, ketamine, phenytoin, and phenobarbital as they can precipitate an acute crisis.
Pathophysiology
- Porphyrins are organic compounds important for the synthesis and activity of heme.
- Porphyrias are a group of hereditary diseases characterized by a partial deficiency in the enzymes involved in heme biosynthesis.1
- Porphyria mutations can occur at any point in the enzymatic pathway, resulting in decreased activity of heme and accumulation of precursors above the affected enzyme. These precursors are colorless and nonfluorescent porphyrinogens. Irreversible oxidation of these porphyrinogens causes the formation of highly reactive oxidants.2
- Accumulation of these precursors can result in cutaneous photosensitivity and neurovisceral toxicity.2
Presentation
- Porphyrias usually occur between the ages of 15 to 40 years and is 4 times more likely in females.3
- It can be classified into 2 categories: acute/hepatic and nonacute/nonhepatic.

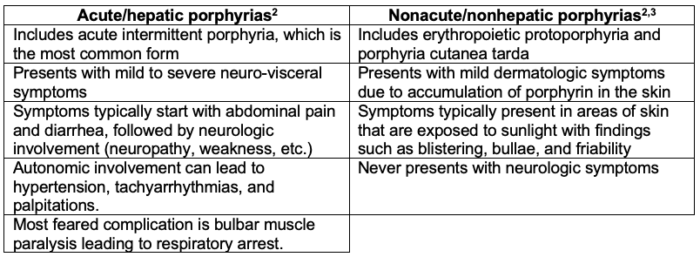
Table 1. Porphyrias Categories
Triggers1,3
- Most drugs that can precipitate a crisis have effects on the cytochrome P450 enzymes and result in an upregulation of heme biosynthesis.
- Calorie restriction, diets that exclude carbohydrates, and prolonged states of fasting
- Large amounts of alcohol consumption, usually binging
- Physiological stressors such as infection
- Variations in sex hormone concentrations (i.e., menstrual cycle and pregnancy)
Anesthetic Management
- For patients with nonacute porphyrias:
- No change in anesthetic management is required.
- If there are active dermatologic lesions, these areas should be well padded and any irritants should be avoided, if possible.
- For patients with acute porphyrias:
- Both general anesthesia and regional/neuraxial anesthesia have been used safely.1,2
- Prolonged fasting should be avoided. Clear carbohydrate liquids up until two hours of surgery should be encouraged and dextrose-containing fluids should be used.3
- Perioperative stress should be treated with appropriate premedication and pain should be adequately controlled during the postoperative period.
- Anesthetic drugs that should be avoided include barbiturates, diazepam, etomidate, ketamine, phenytoin, and phenobarbital.
- In obstetric patients, early epidural placement should be considered.3
- Treatment of an acute crisis includes cardiorespiratory monitoring, treatment of abdominal pain/nausea/vomiting, hydration, monitoring of electrolytes, and administration of heme arginate, if necessary. Urine δ-amino levulinic acid (ALA) and porphobilinogen (PBG) levels should be sent for analysis.1,2
References
- James MFM, Hift RJ. Porphyrias. Br J Anaesth. 2000; 85:143-53. Link
- Jensen NF, Fiddler DS, Striepe V. Anesthetic considerations in porphyrias. Anesth Analg. 1995; 80(3): 591-599. PubMed
- Wilson-Baig N, Badminton M, Schulenburg-Brand D. Acute hepatic porphyria and anaesthesia: a practical approach to the prevention and management of acute neurovisceral attacks. BJA Educ. 2021; 21(2):66-74. PubMed
Other References
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.