Key Points
- Epiglottitis is typically a bacterial infection commonly caused by Hemophilus influenzae type B, which causes inflammation of the epiglottis resulting in upper airway obstruction.
- Croup or laryngotracheobronchitis is a viral infection commonly caused by parainfluenza virus leading to upper airway obstruction and stridor.
- There are key differences between the two diseases, including age, clinical presentation, and management.
Epiglottitis
- Epiglottitis refers to an inflammation of the epiglottis, arytenoids, aryepiglottic folds, and surrounding supraglottic structures. Acute epiglottitis is frequently a bacterial infection, most commonly caused by Hemophilus influenzae type B.1 Less frequently, epiglottitis can be caused by noninfectious causes, such as caustic ingestions, burns, and local trauma.
- Acute epiglottitis was classically observed in children 3-6 years old; however, since the widespread immunization with H. influenzae b (Hib) vaccine in children, the incidence has drastically decreased in the United States. Other causative organisms include Streptococcus pneumonia, Staphylococcus aureus, nontypeable H. influenzae, H. parainfluenzae, beta-hemolytic streptococci, Branhamella catarrhalis, and Klebsiella pneumoniae.1
- Once infected, the bacteria colonize the nasopharynx, which spreads to produce inflammation of the epiglottis, vallecula, aryepiglottic folds, and lateral ventricles.1 Progressive edema and swelling of the epiglottis and adjacent supraglottic structures can lead to life-threatening airway obstruction.
- Patients present with fever, sore throat, muffled voice, and the classic 3 Ds: dysphagia, drooling, and distress (inspiratory stridor). They often assume the tripod sitting position (trunk leaning forward, neck hyperextended, and chin thrust forward) and may be reluctant to lie down.
- Epiglottitis is a clinical diagnosis but can be confirmed with a lateral x-ray of the head and neck demonstrating the classic “thumb sign” (Figure 1).1,2
- The differential diagnosis includes croup, bacterial tracheitis, Ludwig angina, foreign body aspiration, retropharyngeal abscess, infectious mononucleosis, diphtheria, etc.


Figure 1. Lateral x-ray of a child demonstrating thickened epiglottis and “thumb” sign. Case courtesy of Jonathan Muldermans. Radiopaedia.org, rID:54890. Link
Anesthetic Management
- If epiglottitis is suspected, the patient should be transferred to the operating room (OR) for endotracheal intubation in a controlled setting.
- Premedication by any route should be avoided. Oral premedication cannot be swallowed and will upset the child, risking complete airway obstruction. Intramuscular injection is painful, and intravenous (IV) access should not be attempted preoperatively.
- Pediatric difficult airway equipment (different blades, bougie, stylets, video laryngoscope, etc.) and various sizes of endotracheal tubes (ETT) should be readily available in the OR.
- Call for additional help to assist with airway management. The ENT surgeon should be available to perform a rigid bronchoscopy or an emergency tracheostomy if intubation is not possible.
- The patient should be kept as calm as possible.
- Pulse oximetry should be applied and a slow inhalational induction should be performed with 100% oxygen in the sitting position with maintenance of spontaneous respirations. After induction, monitors should be applied and then an IV catheter inserted. Atropine or glycopyrrolate may be administered for secretions or bradyarrhythmia.
- Endotracheal intubation should be performed by the most experienced clinician available.
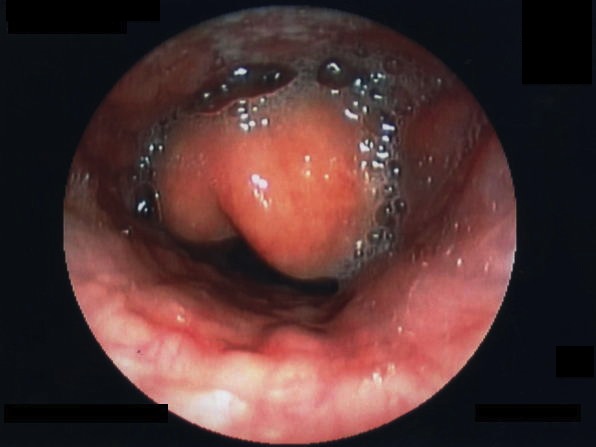
- Direct or video laryngoscopy should not be attempted until a sufficient plane of anesthesia has been achieved. Laryngoscopy typically shows a swollen “cherry red” epiglottis (Figure 2). Confirm endotracheal placement with capnography.2
- Cultures should be obtained to identify the causative organism.
- Following intubation, IV sedation should be administered and the patient should be transferred to the ICU. The patient should be treated with antibiotics, steroids, humidified oxygen, and racemic epinephrine. Patients are usually intubated for 24 to 48hrs.2
- The patient may be extubated after edema subsides and a leak is observed around the ETT. Preparation should be made for immediate reintubation, if necessary.
{kind=link}
Croup
- Croup is a respiratory illness characterized by inspiratory stridor, barking cough, and hoarseness resulting from inflammation in the larynx and subglottic region. The spectrum of croup includes laryngotracheitis, laryngotracheobronchitis, and laryngotracheobronchopneumonitis.3
- Croup is typically a self-limited viral illness that affects children 6 months to 3 years of age. It is most commonly caused by parainfluenza virus type 1 (75% of causes). Other viruses causing croup include influenza A and B, respiratory syncytial virus, measles, and adenovirus. Croup is rarely caused by a bacterial infection.
- Most cases of croup occur in the fall or early winter, and in the United States, it accounts for about 7% of hospitalizations in children younger than five years.
- A “seal-like barking” cough is the hallmark of croup.3 The typical presentation is 1-2 days of upper respiratory infection, followed by barking cough and stridor. Low-grade fever may be present, but unlike epiglottitis, drooling or dysphagia is usually absent. More than 85% of the children presenting with croup have mild symptoms and less than 1% of cases have severe croup.3
- The differential diagnosis for croup includes foreign body aspiration, bacterial tracheitis, peritonsillar/retropharyngeal abscess, angioneurotic edema, hemangioma, etc.
- Croup is a clinical diagnosis that can be confirmed with an x-ray demonstrating the classic “steeple” sign (Figure 3).

Figure 3. Anterior-posterior x-ray showing narrowing of the subglottic airway- “steeple” sign. Case courtesy of Liam Pugh. Radiopaedia.org, rID:53949. Link
- The treatment of croup depends on the severity of symptoms.3 Patients with mild croup are treated as outpatients with supportive care (antipyretics, cool mist, etc.) and a single dose of dexamethasone. Patients with moderate or severe croup are given humidified oxygen, nebulized epinephrine, and dexamethasone.3
Patients with croup rarely require endotracheal intubation (0.2% of cases), and if needed, an ETT one-half size smaller should be used.3 Indications for endotracheal intubation include progressive respiratory failure with intercostal retractions, fatigue, and central cyanosis.
References
- Guerra AM, Waseem M. Epiglottitis. In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing. 2022. Accessed December 11th, 2022. Link
- Vanderhoek S, Dalesio N, Schwengel D. Chapter 34. Anesthesia for Otorhinolaryngologic Surgery. In: Davis P and Cladis F. Smith’s Anesthesia for Infants and Children, 10th Edition. Elsevier; 2022:917-44.
- Sizar O, Carr B. Croup. In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing. 2022. Accessed December 11th, 2022. PubMed
Copyright Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.